
Retinoscopy Lecture (Video)
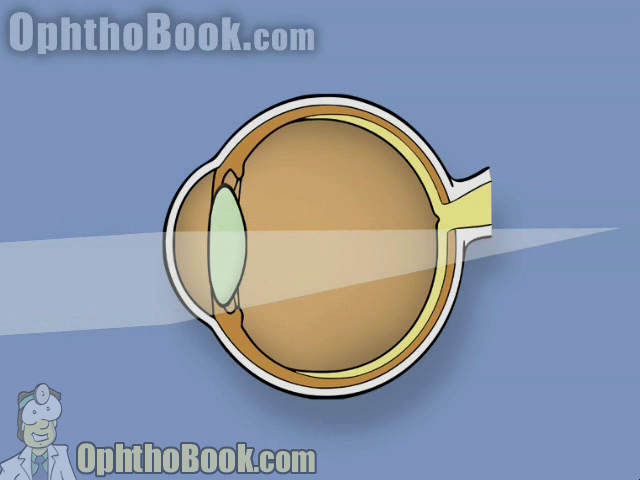
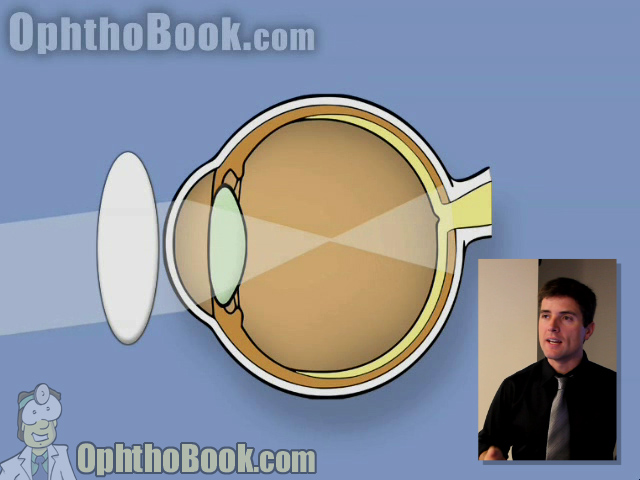
This video lecture describes the process of loose-lens retinoscopy from start to finish. You’ll learn the theory of how retinoscopy works to estimate glasses prescription, then run through 20 different patients with increasing complexity of astigmatism error. This is probably the best presentation on the internet to learn this difficult-to-learn skill:
ScreenShots/Notes from this Lecture:
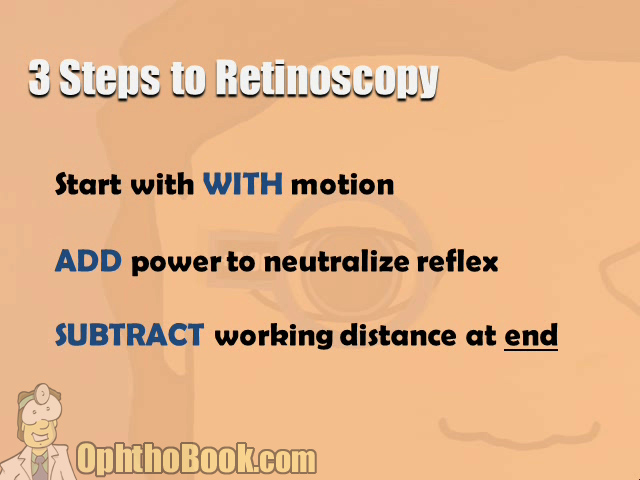
Three Steps to Retinoscopy
1. Start with WITH motion
You need to the retina reflection to be “with” in all directions. If you see “against” motion in the beginning, you might need to hold up a -2.00, -4.00, or even a -10.00 lens in front of the eyes to get that “with” motion. Only then can you proceed without getting confused!!!
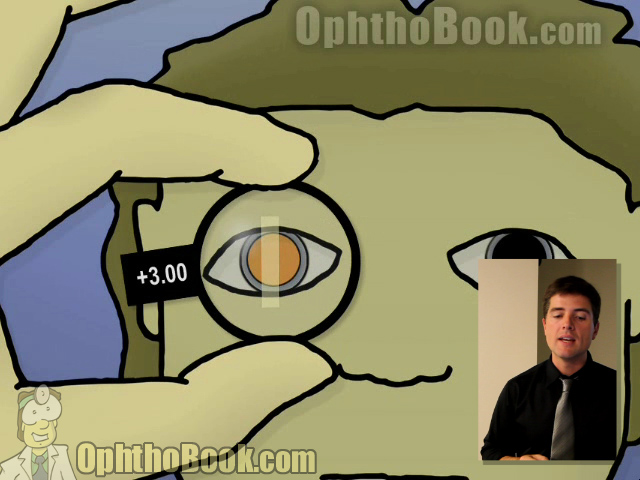
2. ADD power to neutralize reflex
Slowly add more power (plus power) until you neutralize the red-reflex. If you see “against” motion, you’ve gone too far. If the patient has astigmatism, you may get different powers for each axis … don’t worry. Just set the lenses aside so you can calculate the prescription later. Remember: the sphere power is your first lens, the cylinder power is the difference between the lenses. The axis is the angle your light beam ends up at (see example below)
3. SUBTRACT working distance at end
The last step is to subtract -1.50 from the sphere.

Best explanation I have ever had on this topic, (I don’t know how many attempts I made to learn the retinoscopy in observing my prof)
thanks!!
Margherita Montali
p.s. only a question: can you determine accurately the axis with the retinoscopy?
I mean how can you be sure than what are you measuring, for example, in an axis of 60° instead of 70°? Because, I notice, in the prescription of glasses, normally the patient can appreciate a difference of 10°.
During retinoscopy to find the astigmatism angle i.e parallel to trail frame’s angle
Thanks Dr. Montali,
In answer to your question … no, I can’t always tell the exact axis using retinoscopy, though we can often get close.
If I have an adult (who might notice these subtle axis issues) than I can usually get them up to the phoropter anyway. I start with my retinoscopy estimation, then using the phoropter I tweak my power and axis to the exact prescription.
In kids, I just do the best I can and trust my retinoscopy. I like to put my final prescription in a trial frame to make sure the kid likes it (if old enough). Good luck!
-Tim Root
Thanks Dr. Root,
yes I see.
Can I take up your time once again?
When I was student (in Italy), my prof told me it was the best technique to measure the refractives troubles. Now I am in Switzerland, and I continue to be surprise they prefer do another kind of measuration: once obtained the cycloplegia they use the autorefratometer.
What do you think about?
Best,
Margherita M.
The autorefractor is fine … we use it in our clinic prior to refracting new patients and children (if old enough). It gives a good place to start before manifest refraction with the phoropter. Plus, technicians can use the autorefractor with minimal training.
However, you can’t autorefract everyone … including young children, wheel-chair patients, or the demented. Also, the autorefractor is sometimes wrong or the machine refuses to take a good reading. In these cases, loose-lens refraction is the only way to go.
Brilliant approach, thanks so much. You are really making a difference in the ophthalmic education of many people across the world.
From the content point of view it look very good. Till I not seen the video.
AK Singh
FAculty Optometrist
Quality Control Manager
Can you explain how to do it if you use minus cylinders only
DR.ROOT
THANK FOR WONDERFUL EXPLANATION ABOUT RETINOSCOPY.AS OPHTHALOMOLGIST ETHIER WE DEPEND ON AUTOREF OR ON OPTOM ,BUT AFTER THIS AND WITH GOOD PRACTIVE WE ABLE TO GIVE CORRECT CORRECTION.
Fantastic! Best instruction on this topic that I have seen! Many thanks, David
the video was good and simple to understand, however we at the moment in classess work, slightly different to whats on the video, for exmple, we choose the most positive value between the two values as a sphere, then we use a negative cycl to correct for the astigmatism with axis at the positive sphere. however in this video, what type of technique is being used in the video positive cycl form or negtative, as im getting the impression its positive cycl form.
for example: we have two different meridian powers
+4.00 axis90 and +2.00 axis 180
+4.00/-2.00/x90
subtract wrokin distance
+5.50/-2.00×90
thats how we work it out
Thank you very much
It is very nice lecture
thanks very much.i am a begining resident &i admired it very much .thanks again.
I cannot express my great thanks for your wonderful teaching talent
THNX Dr.DAVID.. UR LECTURE IS REALLY HELPFUL…
a small query. wud b kind of u if u cud reply…
how do u select the the axis for spherical power from which the workin distance is subtracted in case of un-rule astigmatism? is it the first one whichever gives complete bright red reflex?
THNX Dr.TIMOTHY UR LECTURE IS REALLY HELPFUL…
a small query. wud b kind of u if u cud reply…
how do u select the the axis for spherical power from which the workin distance is subtracted in case of un-rule astigmatism? is it the first one whichever gives complete bright red reflex?
Thanks alot Dr. Tim. I’m an under grad and this video has become the standard study material for retinoscopy amongst all my friends. Have also seen all of your other videos. you made optha easy and interesting.
How do I get the audio portion to work? Am I required to purchase a video? Can I just buy a download?
thanks!!
Lynn S
it was a very good demo.thank u so much.but i would like to know how u would do it in a keratoconus patient and how to appreciate oil drop reflex.
thank u
Big ( Thank you ) Dr. amazing,
very interesting very nice very informant video. and for all your videos.
I’m not sure of the last two cases
Brilliant lecture Dr Root. I think the best way to learn retinoscopy is using a practice model eye which you can make out of a toilet roll! Please contact me and I will send you some photos and more details.
Clive Novis (South Africa)
could never have understood retinoscopy without this video..u’ve made it so understandabl that i’m so mch interested in smthn i earlier dreaded..
Today as i did retinoscopy fr d 1st time,i cn only thank u fr d knowledge u’ve given..Thank u so vry mch..lukn fwd to more of sch videos..obliged to b ur student..
al d best!!
you are making difference to many people thank you very much i am from Egypt and i have learned a lot thank you again .
iam an optometrist , i was see the vidoeo really iam fine . this teaching is not neglect in my life . thank u
very good vedio. I am student optometry. do you can help me at search about miyopia
its awesome..thank you so much..it was a great help..:)
hello doctor,
Greetings from India. Thanks for the exhaustive explanation. very easy to understand ‘FINALLY’ .i will be looking forward to see many of your videos and lectures.
Thank you
hello doctor,
Greetings from India. Thanks for the exhaustive explanation. very easy to understand ‘FINALLY’ .i will be looking forward to see many of your videos and lectures.
Thank you
i am vitreo-retina consultanat
very nice and informative lecture with easy steps and less confusion
hello..i have questions:
how the distance between instrument and patient’s eye?
what object seen by patient? & how the distance?
the the last one how if i want to use minus cylinder, any different method?
thanks
I,m a beginner from srilanka.i,m interesting about your explanation and need to be a professional in the trade and want some more information about retinoscopy.
excellent lecture i am passing on this site to my fellow techs. I have switched from a + cyl phoropter to – cyl, how do i find the astigmatic power now?
thank you
Rodney in Boston
Thank you for this lectures>>>iwant from you to increased your
vedio about astigmatism.finally thank you.
How about cylinder retinoscopy.Can u explain or discuss it.
thank you
Excellent demo
Dear Dr. Root.
You said the word “ALONG”the meridian right? so you need to convert it to ÄXIS” so if its along 90 or @ 90 and the AXIS would be 180? am I right? I’m sorry but I’m a little bit confused, as according to the book, they use the term “@”or ÄLONG” then should convert it to axis.
Hoping for a quick respond regarding on this matter.
Best Regards,
Mark
Mark,
In this video … I am using the “@” sign to mean “at.” In retrospect, perhaps I should have used the more traditional “x” sign or just spelled out “at” but I didn’t.
I wouldn’t focus on the words ALONG or AT if I were you. As long as you remember that power and axis are 90 degrees from each other, you should be ok.
Tim Root
Hello Dr Root,
Thank you so much for your AMAZING videos! They really help understand concepts from our ophthalmic technician training course!
My doctor prefers minus cylinder, do you have instructions for doing retinoscopy in minus cylinder?
Marissa
It was a really educational video. I really got a better knowledge at retinascopy. Thank you so much.
Marissa,
Most optometrists work in minus cylinder (which is fine). I’m not used to working in minus cylinder, however, so I don’t plan on making a minus video instruction (these videos take forever to put together). Thanks!
Thanks alot Dr Root Excellent practical demonstration for learners as well as professionals.
Dr KHAN
Dear Dr. Root,
Ive always believed reading up from a textbook is entirely different from whats to be practised, which is why I kept forgetting most of the things I read up prior to applying it in real life. Here, your lecture on something this interesting is as close as I could get to a practical experience. I hope to take it forward and learn the most from the foundation you’ve helped me ascertain. Thank you very much.
Regards,
Akansha Sinha.
INDIA
in case of kc how yo see
very easy and understandble
excellent vidéo…
juste i want to ask you , how do the transposition ?
thanks…
Their vidz help me a lot for understanding many things obout ohpthalmology a speciallity that soon i want to doit.. thanks ..greeting from panama!!!
Thank you very much doctor,,
But if i have faster and brighter reflex, is it mean i’m not far to the nuetrilize
very nice video…thank you
Thank you very much doctor. After long time I understood how to do Retinoscopy. This video is very helpful to many Optometrist. Hope to see more of your lectures. Thank you!
Excellent. Concise and positive!
We have a preference for starting with a working distance +1.50, neutralising the most with and then using -ve cyls. The rationale being that it minimises the probability of under-plussing due to the Px (particularly children) accommodating.
…a great lecture and the visuals make this method totally clear.
Thank you.
Brilliant Dr Root
If you work in minus cilinder, jose, you must do the same process.
You can use the second lens to obtain the sphere value(please, don’t forget to substrat 1.50)
The difference between the fist and the second lens is the cylinder. Is always the same absolute value.
And the axis: you can determinate the value
adding or substracting 90
or using the first lens, not the second lens for test the axis
Other way?,…. you can use the Optician tips for convert positive cilinder in negative cylinder.
I’m sorry. I’m spanish and my English is not fluent enough, jose, but if you can speak my language, I could explain it with more detail.
Regards
Gerardo Bellas Spain
it’s very nice.thank u sir
thanks,very nice
Very helpful. All my class-fellows prepared for our final Ophthalmology OSCE from this video. And Dr. Root, you are mad hot! ^_^
great work,,,u r excellent teacher.may GOD bless u
I’ve attempted for several years to learn retinoscopy. I’ve even had a workshop where I thought I finally understood the with and against, however that and no other means of learning ever stuck. It felt like learning calculus … having to memorize complex formulas to apply every step of the way. This is the first explanation/demonstration that flipped the switch on … and it be brightly lit rather than a flickering dimmer bulb that even moths weren’t attracted to. It finally makes complete sense. Sense enough that I’m wondering why it was so hard for me to get before. Thanks so much for putting this together! I’m taking my COT in 5 days and this was the last thing for me to learn … the only thing that has been holding me back for years!
Hi Dr,
Firstly excellent video.
2ndly, what do u mean by writing down the
rx as “at [axis in degrees]”?
Is it the same as “X [axis in degrees]”
for example +0.50 +1.00 at 90 = +0.50 +1.00 X 90 ?
Thanks and keep up the awesome vids.
Thank you
hello dr root
some one ask me why we substract sphere only after doing retinoscope
will you please give me the correct answer i should reply to the the person
I just recently did a COT practical exam (computer simulated) and part of the exam was various instructions that you would give to the patients prior to retinoscope and refraction?
1)Is telling the patient to keep both eyes open during retinoscope and refraction a required instruction? I figure since they are behind the phoropter naturally the eye not being looked at the moment would be occluded anyway, since one eye is always retinoscope and refracted first at a time. When one eye is done you go on to the other one and occluded the eye not being looked at. Am I right?
2) Is telling patient to keep both teeth together reguired during retinoscope and refraction?
very simple thank fr videos
thank nd very simple
Marvelous content, thank You !!
thank u lectures.good video
Thank you very much………its verys usefull…♡♥
Nice video procedure made easy to understand…
Nice video…
sir this is very supportive lecture i learned more from this video.my weakness is on astigmatism that is when i do retinoscopy on oblique case i get confuse to determine the actual axis so. can u plz add more videos for astigmatisam.plz add more videos for how to use jackson cross cylinder to find out the axis of prescription glasses .
thanks,sir
for the wonderful class,iam a resident from india.any videos regarding indirect ophthalmoscope ,perimetry, ffa kindly post it sir
excellent…
but I can’t download the file completely. is it possible to send it to my E mail address.
this was very helpful. Auther is really able to teach well.could be follwed easily.thank you
Retinoscopy made very simple and practical .Thanks Root!
Thank you very much
Hi Dr Root,
Would the prescription of practitioner affect the working distance?
I am with +1.50. If my working distance is 67cm, will there be any effect?
Wendy
When correcting the astigmatism (2nd Axis) in your example, are you using spherical lenses, or, cylindrical lenses placed at the axis of the direction of light?
i have doubt
how to appreciate the brightness of reflex in media opacity
Dear Dr Root,
I’m a french student in Optometry who’s trying to grow up his comprehension in Ophtalmology.
First of all I would like to thank you for the great and really complete job you made which is helping me a lot in my studies. (Website and book)
I have one question remaining about this topic : I was wondering if starting with “against” reflects in both axis couldn’t be better for inhibate the subject’s accommodation and find the most convex prescription than starting with “with” reflect. Can you help me to make the good choice with your experience ?
Thanks again for all your helpfull work all around the world.
Vincent Carpentier
thank you very mch avery useful lecture
Good effort
Oh, such a brilliant explanation!!! Thank you so much!!!
I had a problem to find something similar in russian language, but was lucky to find yours.
Give more examples for this, like -ve sphere & -ve sphere,-ve sphere &+ve sphere,low -ve & high +ve,high -ve & low +ve sphere s
Amazing tutorial, especially for residents starting out. Will always refer to it.
I would like to know how to do retisnoscope and settle on minus cly.
thank u so much Dr. Root for this Amazing video.
i just wanna ask a question that in which cases we can find scissor reflex other than keratoconus?
really beautiful and simple to understand how to perform a retinoscopy
thank you
Great explanation
HI,
I love your lecture. Just curious when working with a phoropter do we still take the difference of the sphere and cyl power to come up with the final cyl. power or do you document the cyl. that shows on the phoropter when working with (+) cyl.
The phoropter already does the calculation for you … you just document the cyl that shows up on the machine.
It was very helpful .now I can actually see something by using the retinoscope,as they say the eye can not see what the mind doesn’t know.
Amazing presentation …after so many years practicing ophthalmology I have rarely seen such an explanatory and easy learning presentation the credits are with Tim root for sharing this with us
Very efficient, informative lecture! I just want to clarify, is it essential to dilate the pupils prior to Retinoscopy? Bcos in our setting, my seniors don’t usually dilate pts that are for retinoscopy. They simply bring the pt in a dark room in the office and then proceed with the procedure. I just want know if dilating both pupils is the standard. Thank you and more power!
How do we correct for astigmatism
…Am a novice
I am an ophthalmologist tech in a small clinic. My M.D. began teaching me this skill today. I was sooooooo lost at what I was looking at and what I was supposed to do. Your video is VERY informative and now I can go to work tomorrow and practice more on our practice eye! Thankyou!!
WHAT A WONDERFUL EXPLANATION. THANKS A BUNCH.
Optometrist and Opthmologists use -ve cylinders what’s the method for this?
Simple, after you neutralize one meridian, you rotate 90-degrees and look for against motion (since you only have minus cylinder lenses to work with). If you find with motion, that now becomes your principal meridian…