
Eye Trauma Lecture
This video lecture from OphthoBook, covers common eye trauma like corneal abrasions, lid lacerations, and globe rupture. If you want to see more of these lectures, click here for the entire series.
This lecture is one of the longer videos in this series, but I think you’ll find it worth your time. I’ve presented a number of common ocular traumas that we see in ophthalmology (from corneal abrasions, to eyelid repair, open globe, lateral canthotomy, hyphema, and iritis). Each of these conditions I’ve captured on video, and so this presentation is very multimedia driven. Below you’ll see some of the captured snapshots.
Screen Captures from this Video:
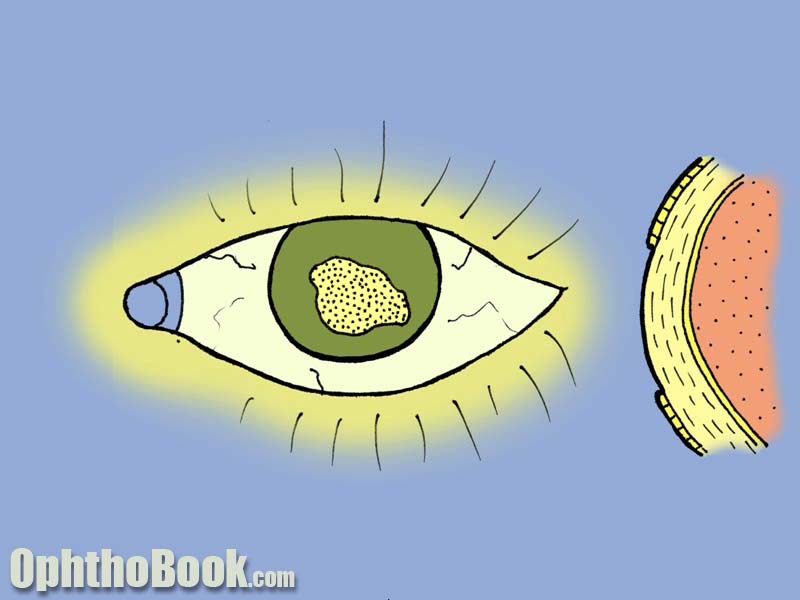 This graphic shows the epithelial loss of corneal abrasion. The cornea has 5 layers, and it’s the surface epithelial layer that is so easily rubbed off. Fortunately, this layer also regrows and heals quickly.
This graphic shows the epithelial loss of corneal abrasion. The cornea has 5 layers, and it’s the surface epithelial layer that is so easily rubbed off. Fortunately, this layer also regrows and heals quickly.
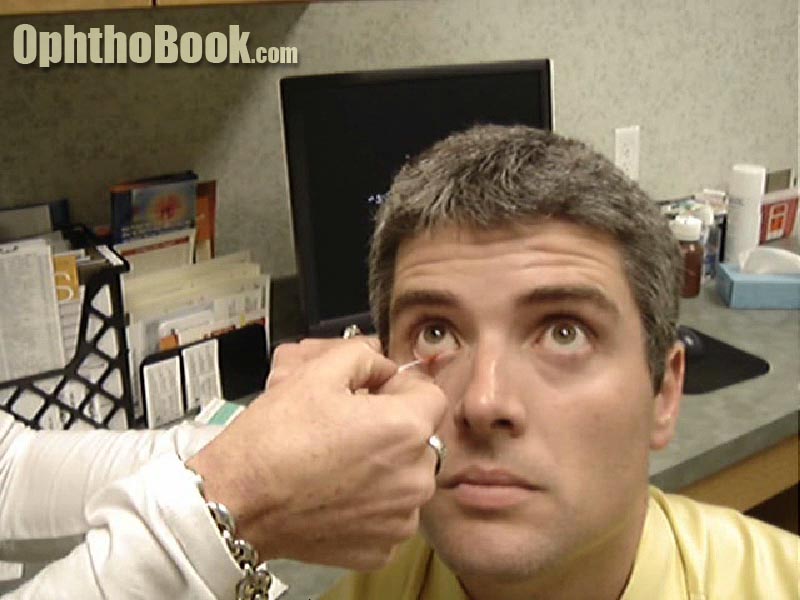 Fleuroscein strips make it easier to check for corneal staining. Regular dye drops work well, but the fluid tends to pool at the bottom of the eyelid and makes spotting small abrasions difficult. Sometimes “less” dye is better.
Fleuroscein strips make it easier to check for corneal staining. Regular dye drops work well, but the fluid tends to pool at the bottom of the eyelid and makes spotting small abrasions difficult. Sometimes “less” dye is better.

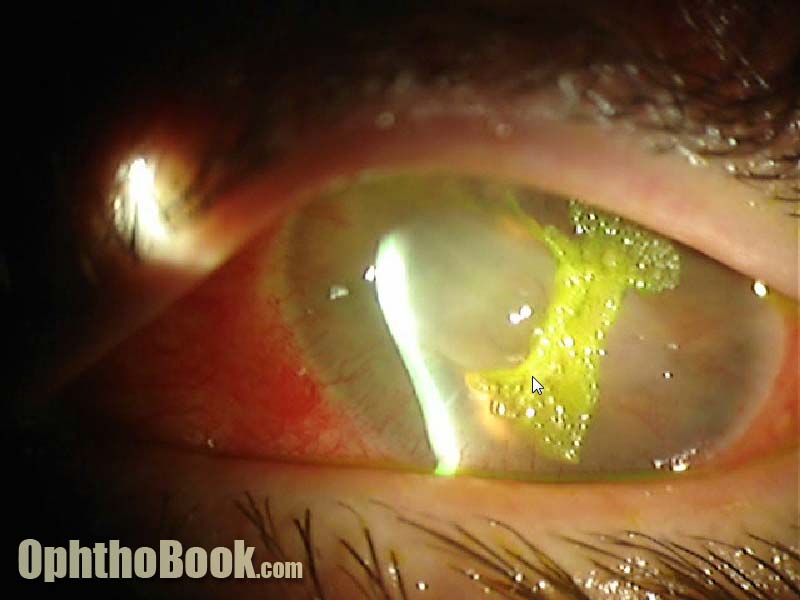
The Seidel Test for finding corneal laceration. This involves rubbing a strip of fleuroscein paper over a potentially leaking corneal wound to detect aqueous egress.

Creating a dermabond patch to stop corneal leaks. This is an uncommon technique that I’ve used with good success on occasion.
Corneal glue for a perforated cornea. I find this material hard to use.
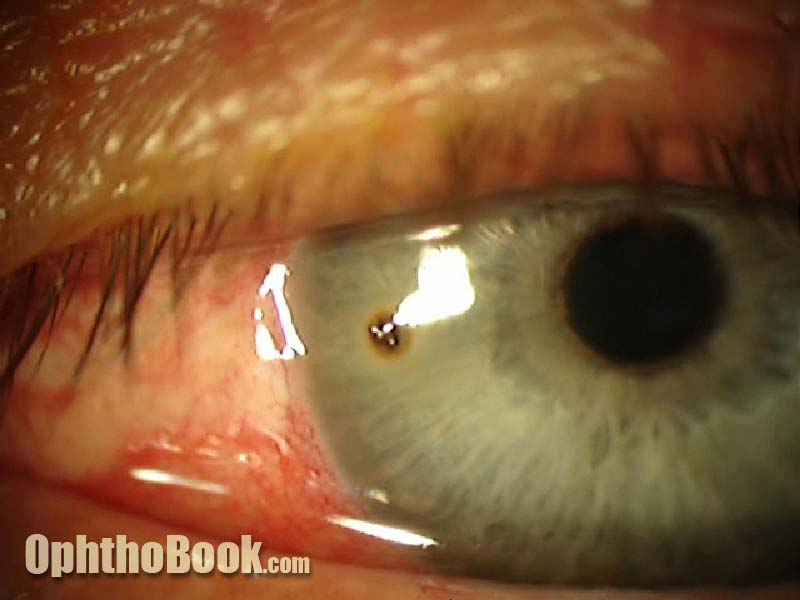
A metal foreign body on the cornea. This finding is very common, and I see several patients a week with metal flakes stuck on the corneal surface. Many of these patients are grinding metal … usually wearing protective eyeglasses. The metal bits seem to get in their hair, then fall into the eye later and rust into place.

KPro corneal transplant after chemical burn. These prostetic corneas work, and are sometimes the only option after failed corneal grafts.
 Checking the pH value after a chemical burn is important. Debris trapped in the fornices (under the eyelid) can cause continous pH imbalance, so keep checking.
Checking the pH value after a chemical burn is important. Debris trapped in the fornices (under the eyelid) can cause continous pH imbalance, so keep checking.

A subconjunctival hemorrhage looks impressive, but is almost always harmless pooling of blood under the skin. They go away after a week or so.
 Dellen of the cornea from conjunctival hematoma. These occur when the conjunctiva swells (such as from a SCH hematoma or bad chemosis) such that an area of the cornea begins to dry. Classically, seen with thinning of the cornea without gross dye staining.
Dellen of the cornea from conjunctival hematoma. These occur when the conjunctiva swells (such as from a SCH hematoma or bad chemosis) such that an area of the cornea begins to dry. Classically, seen with thinning of the cornea without gross dye staining.
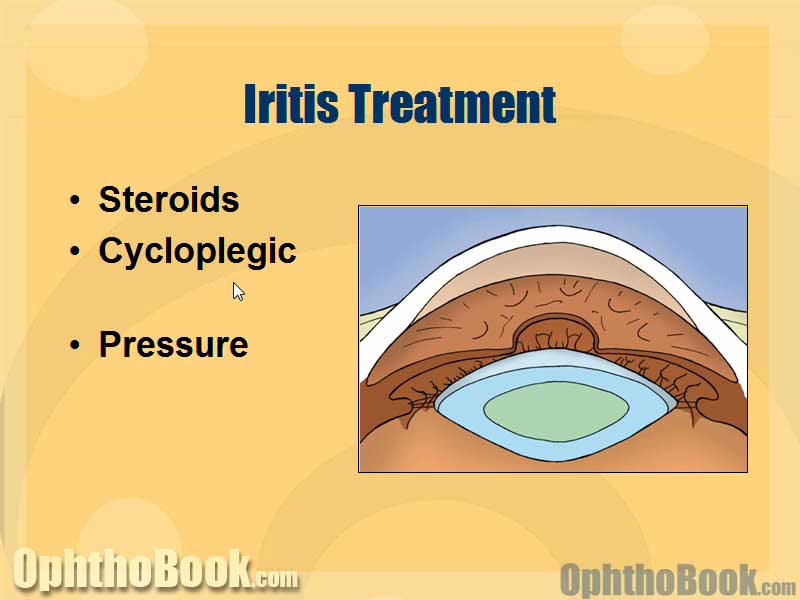
Iritis treatment involves steroids and dilating drops. Steroids get rid of the inflammation, while the dilating drops help with photophobia and help avoid iris synechae.

Hyphema is a layering of blood in the anterior chamber of the eye. A “microhyphema” is when there is blood, but not enough to layer out.
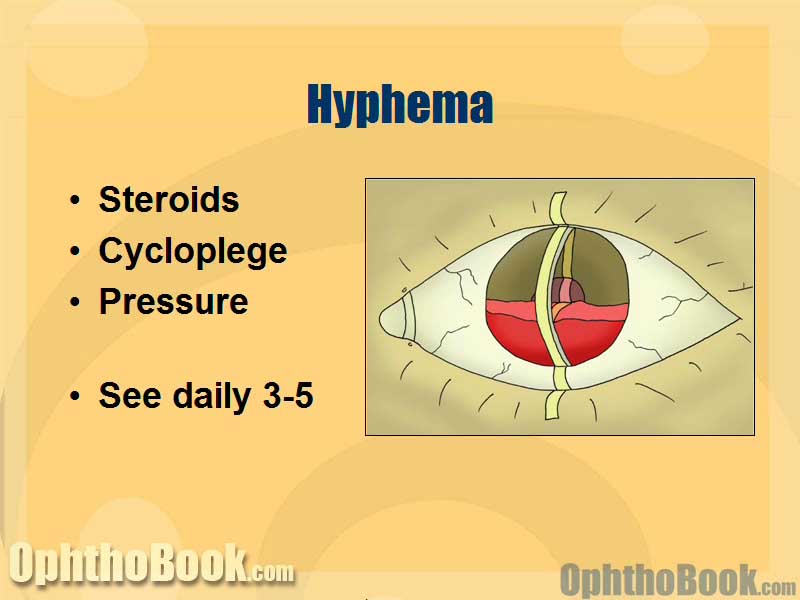 Hyphema is treated similarly to iritis, with steroids and dilators. You need to watch out for pressure spikes … especially around days 3-5, as this is when iris clots begin to retract and rebleeding can occur.
Hyphema is treated similarly to iritis, with steroids and dilators. You need to watch out for pressure spikes … especially around days 3-5, as this is when iris clots begin to retract and rebleeding can occur.
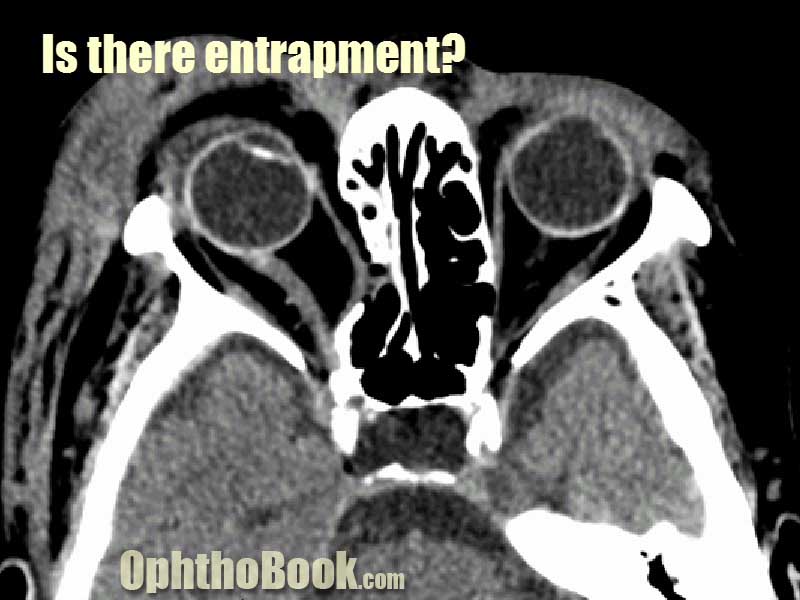 Entrapment of the rectus muscle. This photo shows a medial wall break. The orbital floor is actually the bone that breaks most often.
Entrapment of the rectus muscle. This photo shows a medial wall break. The orbital floor is actually the bone that breaks most often.
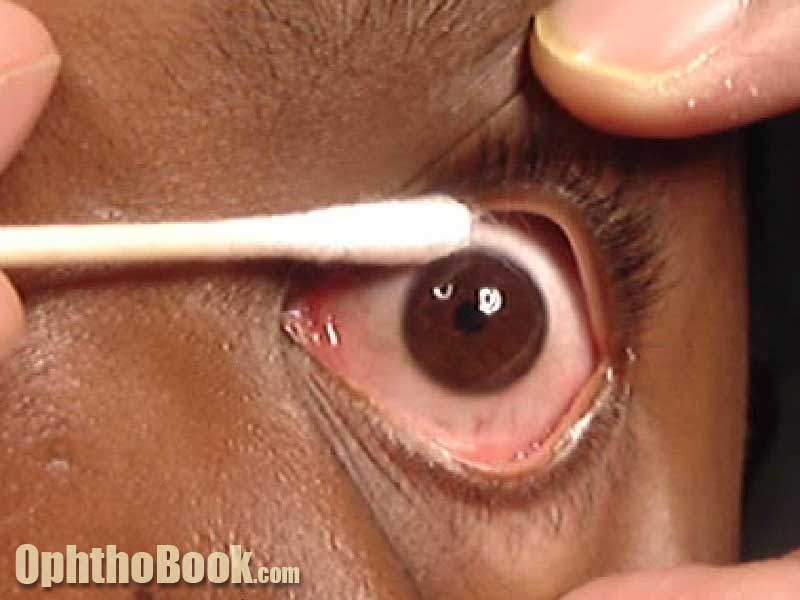 Forced ductions to detect inferior rectus entrapment. This photo shows soft ductions using tetracaine and a q-tip. However, this method has limited utility and you often need to use forceps and grab the eye at the limbus.
Forced ductions to detect inferior rectus entrapment. This photo shows soft ductions using tetracaine and a q-tip. However, this method has limited utility and you often need to use forceps and grab the eye at the limbus.
 Repair of a lid laceration using nylon sutures at the anterior and posterior lamella. You can see the plastic mono-canallicular stent in the punctum at the left edge of this photo.
Repair of a lid laceration using nylon sutures at the anterior and posterior lamella. You can see the plastic mono-canallicular stent in the punctum at the left edge of this photo.
Very informative and fun video!
good hustle! Enyoed it!
Im very interested in becoming an Opthalmologist,I’m in my second semester of college and i was wondering if i could get some feedback on what i need to take in order to start the path of becoming an Opthalmologist….this website really helping me alot to understand the different conditions the eyes has and it helps me understand the work that goes through about performing these operations keep up the good job its really helping.
Hello – is there any way to download this video (or buy) to teach primary care medical residents about ocular trauma? Thanks
Hello,your two new additions to the video collection are really good. Plan to use these for teaching our students.Thanks and keep up your great work.
very nice ,but it will be much more if i can download it
its very clear and great lecture
Thank you very much for sharing your great experience, good speach and super videos!
Its getting real difficult for me to sit n read from my books lately….all thanks to your videos Mr.Root… Thanks a ton 🙂 🙂 !!! Looking forward to view many more of these awesome videos :)!!!
Hi, great website, great work.
The video is not loading from this site or vemo. Anyone else having this trouble?
thanks.
Thank you very much for sharing your great experience, good speech and super videos it is a very good educative video, I like it
thanks a lot, your videos and your explications are really good, and especially very clear: I appreciate the clarity of yours explanations.
Nobody ever made ophthalmology more interesting…
excellent videos and very precise explanation.i wish you will include surgical details which may be of great help for budding ophthalmologist too.
GREAT JOB! WE ENJOY LEARNING FROM YOU
ur videos are awesome.. am new to optho(am a student). our prof had asked us to reads some 25-30 odd pages overnight.. and we had OPD the following day.. u made my work easier.. most of the cases @ OPD were those u have mentioned…!!
thanks again..!
keep the videos coming sir..
I am a resident of ophthalmology at Mayo hospital Lahore in Pakistan.I have learned so much from your videos. Thanks and God bless.
Your videos are awesome!!! I use them in my AF Lectures to excite the class. Thanks
SSgt Smith
Good videos!They help us Ophthalmology students a lot!Thank you!
great and fun video !! you’re the best teacher !!!!!!!!
FANTASTIC LECTURES!! studying ophtalmology is much more interesting now. thanks a lot for your work.
dear sir,
these videos are very helpful for ophthalmic tech;doctors,
thank you,
Tajammalhussain.
very nice lectures, well presented.
thanks for this lecture excellent
This video doesnt play now… I loved all your other lectures!
Excellent lecture ,every body can teach,But only very few people can able to cross the blood CSF barrier,to reach Brain.well you every word can do it,its truly amazing
ليش ما شغال هالفيديو
Hi sir
I’m a GP from IRAN-In middleast- please send this vidio to my email,so i can give it to my other Friends-DOCs- in iran.
in our country mw can NOT Donlowd your VERY NICE & USEFUL & informative VIDEOS 🙁
this is my email address HOPE to….:
drp_allameh@yahoo.com
THANK YOU DEAR DOCTOR.
WITH BEST WISHWES
DR PEYVAND ALLAMEH MD
hi dear dr
I’m optometrist from iran
you are best teacher and your lecture and videos are excellent.
I like have a connection with you through email and consult with you about topic of my thesis.
this is my email address:
(removed to avoid spam harvesting)
thanks a lot dear dr
soraya
Thanks for commenting. I’ll email you Soraya, but I’m pretty busy with other eye projects and may not be too helpful if you have a lot of questions or looking to collaborate on a project.
Great free work
Thank you!!! 🙂
The best ever!! Thank you so much 🙂 I almost feel guilty watching and reading all this for free :O 😉 You gotta great sense of humor too! Hats off Doc!
loved it…
Excellent video! Very informative. Love all of the videos.
simply love this…
Great lecture.
Great lecture, Like it.