
Chapter 8: Common Eye Trauma
When I picked ophthalmology as a career, I never dreamed there would be so many midnight emergency room consults. Little did I know the number of people out there punching each other in the face and slamming their heads into airbags. Armies of welders, construction workers, and industrial cleaners ply their trade without proper eye-protection. Repeated exposure to this trauma can change your world outlook, such that I now dread baseball season, pellet guns, and fireworks. As odd and random as some of these injuries seem, it’s our duty to help these people and save those eyes!
Here are some of the common traumas you’ll likely see coming into an emergency room.
Corneal Abrasions:
The surface of the cornea is covered by a thin layer of epithelium. This “rug” of clear skin is only loosely adherent and is easily scraped off. These surface abrasions are common and we see them daily. The cornea contains more nerve innervation (per surface area) than any other place in the body so these abrasions “hurt like the dickens,” with patients complaining of excruciating pain and intense photophobia. Abrasions are easy to see, even without a microscope, as the raw surface will uptake fleurosceine and glow bright green under a blue light.
Fortunately, abrasions recover quickly and will often completely heal within 24 hours. Until complete epithelial healing you treat with aggressive lubrication and follow these eyes closely to insure the raw wound doesn’t become infected. Many physicians will treat an abrasion with empiric erythromycin ointment as well, reserving more aggressive antibiotics like ciprofloxacin for contact lens wearers and “dirty wounds” caused by tree branches, etc..
If an abrasion does become infected, you’ll see a white infiltrate at the wound. Any abrasion with an infectious infiltrate is officially called a “corneal ulcer.” Depending upon the size and location of an ulcer, you may need to culture the wound and tailor your antibiotic coverage accordingly.
Corneal Lacerations:
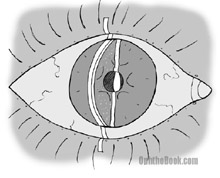
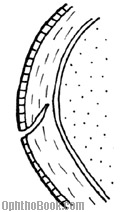 Most corneal scratches only involve the surface epithelial layer. If the injury goes deeper into the stroma, then you have a laceration. With any laceration you want to insure that the cornea hasn’t perforated. You can check corneal integrity with the “Seidel test.” You wipe a strip of fluorescein paper over the wound and see if dye flows down the corneal surface, indicating leaking aqueous fluid.
Most corneal scratches only involve the surface epithelial layer. If the injury goes deeper into the stroma, then you have a laceration. With any laceration you want to insure that the cornea hasn’t perforated. You can check corneal integrity with the “Seidel test.” You wipe a strip of fluorescein paper over the wound and see if dye flows down the corneal surface, indicating leaking aqueous fluid.
If a patient is “Seidel positive” than you have an open-globe injury – time to call in your seniors for possible surgical repair!
Orbital Wall Fractures:
The bony orbital walls are thin and tend to break with blunt impact to the eye. This is especially true of the orbital floor and medial wall. These orbital fractures are common and you will see them weekly (usually at two in the morning).
Tim’s Bumper-Face Theory
 The face is designed like a modern crash-tested car, with many areas designed to crumple and diffuse energy upon violent impact. The sinuses are air-filled crumple zones that protect the brain and other vital structures. When the eye is hit, orbital contents (usually fat) break through and herniate into one of these sinuses. As bad as this sounds, this setup keeps the eye from exploding from high impact pressures.
The face is designed like a modern crash-tested car, with many areas designed to crumple and diffuse energy upon violent impact. The sinuses are air-filled crumple zones that protect the brain and other vital structures. When the eye is hit, orbital contents (usually fat) break through and herniate into one of these sinuses. As bad as this sounds, this setup keeps the eye from exploding from high impact pressures.
Most of the time these orbital bones heal fine with no long-term problems, with patients merely having a great deal of orbital and periorbital swelling that resolves over a few weeks. However, sometimes the broken bone creates a “hinge” or “trapdoor” that entraps fat or extraocular muscles. If there is significant entrapment or enophthalmos, we need to repair the break. During surgery we can release the muscle and bolster the floor to keep orbital contents from herniating back through the defect. This surgery is usually performed by an oculoplastics specialist.
When evaluating orbital fractures, focus on the following exam findings:
1. Vision, color: Make sure the optic nerve isn’t involved.
2. Extraocular movements: Usually decreased from swelling or muscle contusion, but make sure there isn’t any gross muscle entrapment. If concerned, you can perform forced ductions. This involves pulling on the eye with forceps to see if the eye is mobile.
3. Proptosis: Measure the degree of proptosis or enophthalmos using the Hertel exophthalmometer (a fancy ruler).
4. Palpate: Feel along the orbital rim for step-off fractures and subcutaneous emphysema (air crepitus).
5. Sensation: Check sensation of the V1 and V2 sensation on the forehead and cheek. V2 runs along the orbital floor and can be damaged with floor fractures.
Most of these patients do fine and we see them a week later with marked improvement in swelling and motility. In the meantime, you treat empirically with Keflex or Augmentin, advise Afrin nasal spray, and recommend “no nose blowing” (you don’t want to blow air from the sinuses into the orbit).
Lid Lacerations:
 When evaluating lid lacerations, you need to determine if the laceration involves the lid margin and how close the cut is to the canalicular (tear drainage) system. Most of these lid lacerations are straight-forward to repair, though special effort is made to align the lid margins to avoid lid notching and misdirected eyelashes.
When evaluating lid lacerations, you need to determine if the laceration involves the lid margin and how close the cut is to the canalicular (tear drainage) system. Most of these lid lacerations are straight-forward to repair, though special effort is made to align the lid margins to avoid lid notching and misdirected eyelashes.
If the laceration is medial (near the nose) you need to worry about the canalicular tear system – repair of this drain is much more involved and involves threading silicone tubes down into the nose to keep the canaliculus patent.
Metal on Metal:
 Small pieces of metal can fly into the eye – an unfortunate event occurring primarily in welders or construction workers. Particles of metal stick onto the cornea causing small abrasions and discomfort. Metal rusts quickly and will form a rust ring within a day. You can remove metal objects and rust rings at the slit-lamp using a needle. You can also use a small dremel-like drill to drill off the rust-ring. If the rust is deep, or aggressive pursuit seems to be making the situation worse, you can leave the residual rust in place as most of it will eventually migrate to the surface by itself.
Small pieces of metal can fly into the eye – an unfortunate event occurring primarily in welders or construction workers. Particles of metal stick onto the cornea causing small abrasions and discomfort. Metal rusts quickly and will form a rust ring within a day. You can remove metal objects and rust rings at the slit-lamp using a needle. You can also use a small dremel-like drill to drill off the rust-ring. If the rust is deep, or aggressive pursuit seems to be making the situation worse, you can leave the residual rust in place as most of it will eventually migrate to the surface by itself.
Anytime you have metal-striking-metal injuries, you must entertain the possibility of an intraocular foreign body. Small metal fragments can enter the eye at high speed and leave little or no signs of injury. Metal is very toxic to the retina and can kill the retinal cells if not detected. If you have any suspicion for penetrating injury, you should always order a thin-slice CT scan of the head to look for metal pieces not obvious on exam. You want to avoid MRI in this setting to avoid creating a moving projectile inside the eye.
Chemical Injuries:
Household cleaners contain abrasive solvents like bleach and ammonia that are extremely dangerous when splashed into the eye. The first thing you do with any chemical injury is:
Irrigate, Irrigate, Irrigate, Irrigate, Irrigate, Irrigate, Irrigate!
 The final visual outcome for a chemical burn is going to depend upon how quickly the chemical is washed out of the eye. If a patient calls you with a chemical conjunctivitis, tell them to immediately wash their eyes out! If the ER calls you with a chemical conjunctivitis, tell them to start irrigating immediately – several liters in each eye. Then grab your equipment and pH paper and head on down there!
The final visual outcome for a chemical burn is going to depend upon how quickly the chemical is washed out of the eye. If a patient calls you with a chemical conjunctivitis, tell them to immediately wash their eyes out! If the ER calls you with a chemical conjunctivitis, tell them to start irrigating immediately – several liters in each eye. Then grab your equipment and pH paper and head on down there!
Acids are less dangerous than bases as acids tend to precipitate denatured proteins and this limits tissue damage. Bases, on the other hand, just keep on going like the proverbial Energizer Bunny so you need to continually irrigate and check the pH until it normalizes.
On exam you want to carefully check the state of the cornea – hopefully, it is still clear. A red, inflammed conjunctiva is actually a good finding: if the conjunctiva is white, that means its blanched out from extreme damage. Be sure to flip the lids and irrigate/sweep the fornices to remove any material that may be retaining chemicals.
Chemical injuries can lead to significant scarring that may require corneal transplant if bad enough, so you want to be very aggressive with that irrigation!! The emergency room has access to a simple device called a Morgan lens to help irrigate via a suspended saline bag. Little kids hate this thing and have to be restrained when using it.
FUN FACT:
Speaking of abrasives: early Romans used human urine as a mouthwash to brush their teeth. The ammonia has strong cleaning powers. In fact, urine was an important component of toothpaste well into the 1700’s.
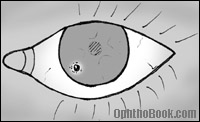
Traumatic Iritis:
 Blunt trauma to the eye can create swelling and inflammation in the front half of the eye. Because the cornea is clear, we have a direct window through which to view the inflammatory cascade. On exam you can actually see “cell and flare” in the anterior chamber. Cells are individual inflammatory cells floating within the aqueous fluid while “flare” is diffuse protein that has escaped through inflamed blood-vessel walls.
Blunt trauma to the eye can create swelling and inflammation in the front half of the eye. Because the cornea is clear, we have a direct window through which to view the inflammatory cascade. On exam you can actually see “cell and flare” in the anterior chamber. Cells are individual inflammatory cells floating within the aqueous fluid while “flare” is diffuse protein that has escaped through inflamed blood-vessel walls.
Patients will complain of painful sensitivity to light secondary to iris/ciliary spasm. Individual cells can be difficult to detect at the slit lamp … and it doesn’t help when the photophobic patient is squeezing their eyes shut and yelling at you. You’ll find it helpful to turn the lights completely off and to make your light beam narrow, bright, and at an angle (like in this drawing).
Fortunately, traumatic iritis generally runs a benign course with resolution of symptoms within a week of treatment. We give these patients topical steroids to decrease inflammation and a cycloplegic to dilate the eye. I generally use a medium-duration dilator like Cyclogyl several times a day – the induced paralysis of the ciliary muscle makes the patient less photophobic. Also, daily dilation forces the inflamed iris to move and keeps it from sticking to the underlying lens.
Hyphema:
 A hyphema describes blood floating in the anterior chamber, a common finding after blunt eye trauma. If the bleed is large, the blood will settle out in a layer at the bottom of the anterior chamber. If the entire AC is filled with blood, you’ll see an “8-ball hyphema.” Most of the time, however, the bleeding is microscopic and can only be seen as “red cells” floating in the aqueous fluid.
A hyphema describes blood floating in the anterior chamber, a common finding after blunt eye trauma. If the bleed is large, the blood will settle out in a layer at the bottom of the anterior chamber. If the entire AC is filled with blood, you’ll see an “8-ball hyphema.” Most of the time, however, the bleeding is microscopic and can only be seen as “red cells” floating in the aqueous fluid.
Blood typically clears well, though you can get staining of the cornea if the blood is persistant or coexists with high eye-pressure. Encourage your patient to sleep with their head elevated (to help the blood settle) and to avoid straining. You typically give steroids (to decrease the inflammatory response) and a cycloplegic dilating drop to help with photophobia. As with iritis, this dilation also keeps the iris from sticking to the underlying lens and forming synechia. With African Americans, consider checking for sickle cell disease. If they do have sickle cell, avoid carbonic anhydrase inhibitors as they cause a local acidosis that worsens sickling.
Follow these patients daily, as the bleeding can get worse. The main danger time is days 3 to 5 because this is when clots can contract and rebleed. You need to monitor their pressure as blood can clog the trabecular meshwork. After the blood has completely resolved and the eye is quiet, perform a thorough gonioscopy exam to access for “angle recession.” This is when the ciliary body splits from the blunt trauma — this is a sign (but not a causative factor) that the patient has also likely suffered trabecular meshwork damage and may eventually develop glaucoma in that eye sometime in the future.
FUN FACT:
 Speaking of fluid layering …
Speaking of fluid layering …
The “black and tan” tradition of beer mixing originated over a thousand years ago when Viking explorers raided the Celtic islands. The Vikings would mix their lighter northern beer with the local dark beers. Later, the term “black and tan” came in use to describe the uniforms worn by cruel British solders sent to Ireland in the early 1920’s to suppress uprisings.
A black and tan is most commonly constructed with Bass Ale (an English bitter) and Guinness (an Irish Dry Stout). The Guinness is pored over the lighter colored beer using an inverted spoon to disperse the Guinness and decrease mixing. The beers have different densities and so will remain “layered.”
The “black and tan” is enjoyed by beer enthusiasts who find a straight stout too harsh. However, you may want to avoid ordering one in Ireland because of its historical relevance.
Open Globe Injuries:
The eye can be perforated many ways … I’ve seen firecracker explosions, gunshot wounds, car wrecks, and domestic accidents that have perforated the eye. Visual outcome is usually terrible and a blind, painful eye may need later enucleation.
If you suspect an open globe injury you need to evaluate the eye in the operating room. One thing to remember – if you suspect an open globe injury, cover the eye with a shield and don’t push on it. You could extrude the eye contents (pop it like a grape) if you push on the eye.
PIMP QUESTIONS
1. You have a contact lens wearer with a small corneal abrasion. He is in excruciating pain and requests that you pressure-patch his eye for comfort. Will this speed up healing?
Patching may speed healing by keeping the eye immobile and lubricated – but you should never patch an abrasion that might fester an infection. Thus, you don’t patch contact lens wearers as you don’t want a pseudomonas infection brewing under that patch! If you decide to patch a patient, you should really follow them daily to make sure they don’t develop an ulcer.
2. What’s the easiest way to see a corneal abrasion? How often do you need to follow simple, non-infected abrasions?
Abrasions are easiest seen with fluorescein under the slit-lamp microscope, though large abrasions can be detected with only a handlight as the edges of the abrasion creates a circular shadow on the iris underneath. You’ll want to measure the epithelial defect and see them often (perhaps daily) until it heals to make sure they don’t become infected.
3. What is the Seidel test?
This is a method to see if a laceration has penetrated completely through the cornea. Basically, you’re using fluorescein to look for leaking aqueous fluid.
4. What findings would prompt you to take a patient with an orbital floor fracture to surgery?
If the patient has muscle entrapment or significant enophthalmos. Most patients have some degree of EOM restriction from soft-tissue swelling. Entrapment causing reflexive bradycardia would also push you toward surgery.
5. What portion of the eyelid do you worry about with lid lacerations?
If the laceration is medial (near the nose) it could involve the tear drainage pathway. These canalicular tears are more complicated to repair.
6. A patient accidentially splashes a large amount of bleach-based cleaner in her eye. What should she do?
Wash it out immediately – the faster, the better!!!! If an ambulance picks her up, have the EMTs irrigate in route, and alert the ER to irrigate her eyes as soon as she hits the door.
7. What is the best way to test the pressure in an eye with a likely open-globe injury: with slit-lamp applanation or with the hand-held tonopen?
If you suspect open globe, you don’t want to be mashing on the eye, so neither of these is correct. This is a trick question … hahahahaha!
8. How often should a patient with a hyphema be seen and why?
These patients need to be seen daily for the first week to check for pressure. This is especially important on post-trauma days 3 – 5 as this is when clots begin to retract and rebleed.
9. An African American presents with hyphema after trauma. What additional workup might you consider? Are there any medications you would avoid?
You may consider getting basic coagulation labs and a sickle prep. Avoid CAIs as these promote acidosis and can worsen sickling of blood in the anterior chamber and worsen glaucoma.
10. What two beers are most commonly used when making a “black and tan.” Which beer goes on top?
A black-and-tan is made with Bass Ale and Guinness Stout – the Guinness goes on top and is usually pored over a spoon to keep it from mixing.
what is recommended for a patient with traumatic iritis whose synechia doesn’t resolve after a week of dialation and steroid drops?
tell me the treatment of blood vessel rupture in sclera
Usually, a subconjunctival bleed is harmless and does not require treatment. The redness will go away in a few weeks.
when is an abrasion likely to progress to recurrent corneal erosion? Symptoms/Treatment of corneal erosion.
when i was young, a guy hit me in the eye with a brick. since then, i having been dealing with one eye, only to see a shadow in the left eye. are there any way to correct this problem. now that i am older, i want to correct this problem, not just so i can have vision, but for cosmetic. right now, because this makes me look cross-eyed.
i saw a trauma case more recently, and sadly, i couldn’t help the young girl. hopefully, after i read this chapter, i will feel more confident and comfortable when i encounter another ophthalmology cases and know exactly when to refer immediately. thanks so much for all of your wonderful efforts and the great use of your talent. by the way, are you planning to create a video for this section or will it be too gruesome?
What is the onset of a foreign body from the moment a metal particle enters the eye till the time it begins to become embeded and the cornea heals over>
i wonder if it is correct to use systemic steroid in order to decrease eye inflammation after trauma ?
Hi Tim,
Your Dad gave me your website address and I have spent the last hour looking at your work.
It is very impressive. I think that your many talents and of course your medical training are strongly evident in this website.
Who in your field could have produced a book and website comparable in quality to this? I think I know the answer. Nobody!!
Keep up the good work Tim, we are all proud of you and your accomplishments.
Uncle Jerry
Nice articles for Practitioners and I found it very useful for myself
WOW! the Eye for Dumbies 🙂 I am a nurse and ran across this site. I am glad I clicked the link. Question…have you seen patients with dystrophy in just one eye? Is this rare? I was recently diagnosed with this in my OS 🙁 or the doctor thinks it could be an unhealed abrasion chronic is a facial trauma. Could you offer some insite to me. Thanks, April
Wow, an intelligent, philanthropic, good looking chap with a sense of humour: are you single?? 🙂
Very useful website, thank you and good luck.
we all like question no.7!! 😛
Fantastic! You make it all sooo interesting! Great cartoons,too. Thanks from all your techs.
Hello. 2 days ago, I was assisting mother-in-law with cleaning her basement. She used a lot of bleach during the cleaning, which created fumes that irritated my eyes. I removed myself from the area after I noticed that my eyes were really tearing up. I patted my eyes; however, I didn’t irrigate them, as I didn’t think it was that serious. Saturday night at about 9 pm, I was driving and noticed that I saw halos around all the lights outside, especially as I got closer to the lights.
I immediately went to the emergency room. My eyes were flushed. I explained to the doctor that my eyes were irritated from the bleach fumes, but not from bleach splashing into my eyes.
Sunday evening, I still see the halos around the lights, but they are not as severe.
The doctor told me that the ‘halo effect’ should go away within about 24 hours of the incident;however, I still see them Sunday night, which is about 32 hours later.
I have a follow-up appointment with the opthamology dept today. However, please provide your expertise with regard to this.
My Grandaughter was hit in the eye 2 days ago her eye was red & tearing ,but this morning she said she is seeing a halo around her eye when she looks at the light .We went to ER,was tokd to see eye Dr. on Monday ..If she got worse go to Philly eye Hosp. for Children..What does this halo mean around the eye?
Four moths ago I got weed killer in my eye, not a splatter but I rubbed the corner, near my nose, with my hand and the the weed killer was on my hand. I rinsed it for a long time, but not near enough I know now, because it still burns four months later like I have soap in my eye. Afterwards, it wasn’t untill several days later that I saw my doctor and he gave me TobraDex ST, which helped a little bit, but the burning pain has not gone away. My question is, after four months, will the pain ever go away?
hi doctor,
m in 2nd yr of optometry
ur book is really a great blessing for optometry students
My son missed his optical bone surgery under his left eye due to fear..he just turned 18 and was prepared to get it done at a later date. When he returned 5 weeks later, he was told they could do nothing. He was told to watch for seizures, dble vision and blindness. We were very upset. He was informed by the triage nurse that he would get it done if he felt ready at a later date. We are crushed. Is there anything / options he can do to fix this? Is surgery really out of the question? Would he really go blind? He still has darknes around the eye…he stll plays video games. We are going for a second opinion. Need to see what options are available for him.
There is a shrivelling at one edge of my cornea. Removal by laser has been recommended. Is there any urgency? Will it spread ? Age 77. Both eyes cataract removed over a year ago.
Why no reaction in 4 weeks? Please e-mail iamcksuri@yahoo.co.in
Got hit it the eye by the end of a snapping bungee cord. Went to the ER. Was totally blind in that eye. I am being monitored. Now two days later still cannot really see, but with the injured eye I can detect a little light now. Doctor cannot see in to evaluate the retina, too clouded, by blood I suppose. Very concerned. Also concerned about the lens. He said it looks like I will gat a cataract from this.
Recently my son got an hit with Cricket Tenis ball in his eye. at First day in investigation, all his scanning of eyes and vision test were done. Everything was found normal with very good vision. However, he showed a good recovery in first 4 days. but on 5th day he had high pressure in eye and had vommitting. This again reveresed the case back.
Further his ozzing is yet going on. He is sleeping in inclined position so as blood keeps moving down with gravity. His earlier dose of Dymox which was 1 in day has been increased to 3 per day. What could be your opioin on this and does having this much dymox will have any side effect. Its more to control currently his eye pressures.
I have a swollen left eye,burns,stings,dry red,gets stuck, twice i saw dark blue spots and my rite eye is red. I went to two doctors, one doctor said my eye looks fine and no reason to see the opthamologist, the second doctor said the same but prescribed Patanol 0.1%. I dont feel any better.I did explain that i got a cream in my left eye that contained some type of berry extraxt to bleach the skin that also had an antiaging igrediant.(it was a sample,did not have specifics.)Im scared that no one is paying attention.I have a migrain headache as well. What should I do?
I am 86 years old, and back when I was 20 , I was injured and I had :”Choroidal ruptuere”,”which had a cresent shape”, is it true that it can change due to age (through 60 years)?
What are the consequences of a child washing their eyes out, over and over, day after day with soap?
Please help my child has OCD and this is a ritual. Her vision is declining and hypersensitivity to light has become an issue.
Im 14 yrs old. One and half month back cricket ball(not leather ball, but a cork ball)hit my left eye, in first instance epitelium layer was out from 2-3 spot and by mediacal aid it was recover within 2 days. but after two days misty imaages were seen, then treatment was followed by ultrasonoigraphy and engiography, while both reports were O.K., but Dr. was suspected to Glucoma and finally confirm after 3-4 days of mediacal tests about one month back(as per him eye injury may followed by Glucoma in many cases but it’s not troublesome). Medicine treatment of Glucoma was started and eye pressure (tension) has been under observation on every ulternate day, and tension was measure between 24 to 29. Finally on 21st of this month Dr. advised for surgery since tension is not getting down even after of one month taking pills and now it may hurts nerves of eye ball resulted slightly vision loss. Then on 23rd I changed the Dr. for better opinion, while tension was measured 34, here Dr. advised for next 15 days on changed medicine. Now I am confused should I continue on medicine or go for surgery? Please please help.
My son bumped his eye, and now he won’t open his eye. We dit go to dr and got eyedrops is it normal.
Hello. This morning I noticed that there was a swelling on the right side of my left eyelid. It is very painful n burns slightly. Yesterday however I was cleaning with bleach and thought probably the fumes that were released might been the cause since I was cleaning in an enclosed area. Can this be the cause? And what should I do to reduce the swelling.
Hi I was in a car accident a year & a half ago whereby I was rear-ended & hit my head on the head rest. I have had problems with my right eye ever since, at times of heightened stress it seems to throb & then I also often get a “snow globe” affect where I see small white particulars floating around. I had a full eye exam & they said that there is nothing They can do except hope it settles down in time? I am 40 years old & have always had great vision & no problems before this.
Many thanks for your reply, Kate
My daughter (15) was hit in the eye with a bad basketball pass pretty hard. She didn’t have any noticeable bleeding or swelling and thought nothing of it, even finished the game. A couple of days later, she noticed when she woke up that morning that the affected eye was ‘slow to wake up.’ She didn’t mention it to me until several days later. It happened again yesterday and she admitted that it has happened a few times since then. Yesterday, it happened in the middle of the day while she was exercising, the rest of the times had been while she was waking from sleep. Any suggestions of what might be going on? I plan to make an appointment with the optomatrist tomorrow.
This morning 12/23/12 I notice in my left eye was red under the lid only in one spot. There is no pain what could this be?
Hi,
I had a blunt eye trauma 2 weeks ago, and orbital floor repair surgery 11days ago. Since the surgery the white of my eye is covered w/blood.
At times looks like it is bleeding.. About 3-4 days ago a portion of it looked a little lighter shade of red.
This morning that lighter shade is almost as red as it was a few days ago.
My DR said my body would absorb the blood. It takes time, it has been over a week with no real progress.
I am worried there is a more serious issue here, could there be?
And if it is truly a waiting game is there anything I can do to help speed up my body’s reabsorbtion of this blood.
Thank you
Amy Wilson
4 years ago I was injured with an exercise band in my right eye. I developed a hyphema and my sphincter muscle was injured. My pupil was irregular and large. I developed a cataract and had that removed and my pupil tied in to appear more regular and smaller. It does not dilate. I have to wear close up lenses now to see print. Before the accident I could read and use the computer without my glasses. I experienced annoying floaters prior to the accident. Now if I take my glasses off and try to look at someone within a few feet or try to read, the injured eye feels irritated and the floaters intensify. Also, when I blink or look at a white or light background, I see many fine lines as if I were looking out of a cracked egg shell. I have followed up every 3 months with opthamologists. None of them can help me with my problem. My eye pressure is elevated in the injured eye and reads about 23 versus 17 in the uninjured eye. My life is not as comfortable as it used to be. It is annoying having to experience this feeling of swelling of the eye and the little lines with lots of floaters in the field of vision especially under bright light conditions. Are my symptoms common with an injury to the sphincter muscle of the eye? What can I do to have a better outlook for the future?
Hi doctor,
After I was punched in the head and my brow area recently, the following next day onwards, my left eye keep seeing a very faint thin almost vertical moving whenver I open my my left eye to see or whenever I blink my left eye?
Do you think this is caused from the punch?
Also what do you think is the problem and what can be dont to rectify it?
Thank for your attention
By the way, is it you reply our queries directly to our email addresses we typed above? (Becos I did not see your replies on the above other questions posted openly here)
Editor: Micheal, you need to see an eye doctor right away. You are most likely suffering from a (normally harmless) a vitreous detachment, but new floaters could also indicate an early retinal detachment (potentially blinding). This can only be diagnosed with a dilated eye exam.
my both eyes have gone inside deeply. How they will got out again and appear normal?
I had a corneal laceration according to a specialist, I keep feeling something on the corner of my upper lid towards my right ear , it bothers me a lot, it is painful and the doctor was concerned because my eye did not heal in one week. It keeps hurting specially at night, I can not lean on my right side because the pain worsens. The Dr. Told me that I have inflamated cells in my cornea, however he does not know why I have reacted like this. What can it be, the light bothers me a lot and this did not happen before. The Dr. Told me that the use of a computer or reading will not affect the healing what is your opinion? I had a bad cornel laceration when I was a child about 7 yrs. old and I had to wear a patch for long time I am not sure for how long, but why if the light bothers me a lot the Dr. Says that it does not make any difference in the healing process! please respond ASAP. I am very concerned about the healing of my eye.
Hello good blog
can blunt force trauma affect the uninjured eye
thanks
I got hit in the eye 2 days ago and since then i noticed that everytime i go into somewhere bright like stepping outside even when its not yet sunny i feel a very sharp pain in the eye even when i quickly close it and touch the eye the pain is still there. What can i use or do
I don’t have insurance. No opthamologist will see me. I went to the ER and they let me discharge with the diagnosis : opthalmoplegia / diplopia.
I just woke up this past Sunday morning and it felt like my eyes were spinning. I came on the web, and seen people had women with similar issues but they went away later in the day. So I waited one day. The next morning I woke up and still I see double. I go to the hospital (6/17/2013) and they do an MRI because I also can’t taste anything. MRI confirmed there’s been no stroke, no MS. Bloodwprk says no diabetes. So as I’m at the hospital I notice that I have very little control over my right eye. I can literally see two different directions.
Now let me back track, for a second. Before Sunday I had an eye infection. I don’t sterilize my make up properly and I’m used to these infections. Usually I use baby shampoo to clean my eyes out because its tear free. I didn’t use baby soap this time. I used two things I shouldn’t have used, peroxide and shampoo. I don’t remember which I used first. I only used the bubbles of the shampoo, & the peroxide I had put a drop on a q-tip. I just wanted to clean my eye lid. Nothing happened for four days. I had normal vision. I started cleaning my eyes with warm sterile salt water, since I could see the chemical burn on my eyelid. This salt water helped with swelling, too. Saturday came, and I didn’t use salt water. My eye had little to no swelling, perfect vision. (Somewhat perfect I have terrible eye sight)
I wake up Sunday unable to see straight. So, the ER refers me to the opthamologist bit she wont see me because I don’t have insurance or $175 dollars for her office visit. I can move my eye sometimes.Sometimes the muscles moving my eye just give out. Will Ibe like this forever or will my eye fix itself? 🙁
Dear sir, my both eyes have gone inside deeply. When I was child,since then my both eyes is going inside slowly. Now They have gone inside deeply. I am looking very dirty. So, please tell me the treatment how they will got out once again and will appear normal.
Hi Doctor,
I was punched in the right eye recently and my vision hasn’t been the same ever since. An MRI and x-ray was performed and I was told there was no fractures.
At first, I was unable to see clearly out of it due to a large scratch on my cornea. I was given various drops; an antibiotic, drops for inflammation, and cyclopentolate to dilate the eye.
I saw a doctor a week ago and was examined and told my eye looks to be healing fine and did not see any issues. My vision has come back for the most part and I stopped taking the drops 2 weeks ago.
However, my right eye remains dilated and I have an issue focusing on near items as well as discomfort in some occasions. It’s most bothersome when I elevate my head and try to shave my neck as I see 2 images and feel a strain on my eye of some sort. This also occurs when looking through my left peripheral in instances while I am driving.
I called the eye center I had visited to see if it may be due to the drops I was taking, but they told me no. They said it was most likely from the eye trauma and might be permanent damage. They also said to give it time to see if it corrects itself.
Is there something I should be doing to help it heal? Can this really be permanent? Is their a procedure to correct this if so? This has left me pretty worried and any feed back you can provide would be highly appreciated.
Thank You,
Amer
I was hit in the side of my head 3 days ago my left eye swelled up and was swallon shut after appying ice every 2 hours it has oponed back up 3 days later is still soar its turning yellow around it now how long until I can open my eye lid up all the way my left side of my nose is numb as well as my three of my front teeth also it itches sometimes where it is numb any advice would greatly help me out thanks.
Hi
I got hit by a shuttlecock 1week ago. Was order bed rest Iin hospital to settle the hyphema. After discharge I still see blurred vision. Latest review is blood clearing. This is 2nd week, Iwoth spectacles the surrounding looks fine but if I look into phone or PCM screen the injured eye cannot see the words is all double image.
Is this normal or the trauma cause difference to my myopia degree?
Josann
Hi,I got hit in the eye recently and now i have rlly bad pain,some times its just plain pain and other times its throbbing pain. i went to the hospital for them to tell me what was happening but it wasnt hurting when they checked me out and they said everything was fine but that i had a dry eye. i put on the drops they sent me but it doesnt help me much? is there any possibility it could be something else?
my grandson had an airbag go off yesterday morning- it hit him in the face and his right eye is very bloodshot, his vision is blurry and he can open his eye half way.
Do I need to take him to the e.r.?
thank you for your input.
Hi Doc,
I have just walked out of E.R and have been told that I might be allergic to something in the air. The thing is for the last couple of days my eye has been irritably itchy. this morning I woke up and went to open my eye and just the sense of a bright light really hurt my eye likewise at night (photophobia) but even seeing bright lights with my opposite cause strife to my left. my eye is that red I can’t really notice my pupil. Doctor cannot find no foreign body, no laceration etc but something with a high blood flow or something with the blood vessels. Do you have an idea what I might have?
My question actually the past 3days my left eye started becoming a little sensitive and I thought it will pass but this morning when I woke and opened my eyes a watery substance came out my left eye when it opened,the colour of my eye inside was not white as it should be but it looked more light brown if I can say so,I bought eye gene but its not helping what do U think it can be I did not hurt my eye So I would really like to know what it could be and what to do…Please and thanks.
I had an eye injury over 1 year ago. had a flake of metal 3mm long 1mm thick enter front of eye and just about exited the rear. I had it removed that day and my lens. My surgeon fitted some sort of gas bubble in eye to support the rectna. after the eye healed and bubble dissolved I had a rigid contact lens made. When I put len on I noticed I have diplopia (double vision) They tried correcting it prism glasses however they didnt work. went and saw eye muscular specialist. He fitted me with stronger prisms however this was the results. If I concentrated on something I could see singlely however whenever i turned my head while keeping eye on object it went back to double. everytime I blinked it slowly went from double to single. My vision in the injury eye with a contact is very good however they cant get them working together. he said to me it a 50% chance it could go better or completely worse. So now i have a blurred (no contact in) double vision constantly which is very annoying. With my contact in without prisms I have single vision up close. I do not understand why I have it and the doctors seem bit confused at the whole matter.
Have you ever heard of this happening to anyone else? Is there anything else I can try? Eye transplant?
Rueben,
Your case is impossible to comment on in this format, but I’ll make a couple of observations:
1. It is difficult to get the eyes to work together when one is aphakic (has no lens or implant inside). Image disparity between the eyes make it harder for the brain to fuse two images from your eyes into a single picture in the brain.
2. You have had an injury that affects the muscle control of eye movement. In these cases, prism can improve diplopia. However, prism may NOT be able to eliminate the double vision in every direction of gaze. The goal for strabismus doctors is to decrease double vision in primary gaze (looking straight ahead) and with reading, as this is the most important for everyday activity.
3. Near vision is quite different than distance vision. Many cross-eyed people have no double-vision at near because the eyes are “supposed” to cross a little when looking at near objects. Many people require a separate prism glass for both distance and near.
Good luck. I would give it time. Given the trauma you went through, I am amazed that you have any vision at all. There isn’t much else to try other than seeing a different strabismus doctor for another opinion.
I touch my lens with dirty hand and its 7 days gone but still I cant use it. Its irritating. How can I clean my lens and use it again
Hello,
My little boy accidently scratched my eye and I could not sleep the night it happened because when I blinked or closed my eye it really hurt. I seen the Doc and he said it has already started healing but that was like 4 months ago and every other night since I have woken up early in the morning feeling that stinging pain from the scratch but this time if I shut my eye for around 15 mins the pain dissapears and I carry on as normal. Do you have an explanation for this?
Danny, sounds like a recurrent corneal erosion. More details here:
http://www.rooteyedictionary.com/recurrent-erosion/
When I go swimming for a long time once I get out I see a halo effect but that is just from the long exposure to chlorine on the eyes my right eye clears up after several hours and then my left eye clears up after 24 hours.
This is really good and educating
Pls let it continue