
Chapter 9: Introduction to Optics
Before I started my ophthalmology residency I didn’t know a thing about optics. It was embarrassing during my internship year when friends would ask me to renew their glasses only to discover I hadn’t a clue as to how to decipher their prescription!
Optics principles are easy to grasp, but I think you’ll find it difficult for these concepts to permanently “sink into your brain“ until exposed to this stuff on a daily basis. Nevertheless, a review at this point is useful. These are the basics I wish I’d known before my first month as a “prescription-writing resident.”
Myopia and Hyperopia
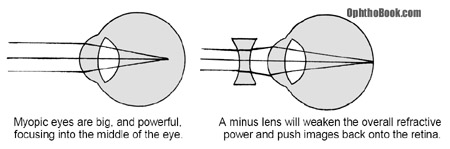
A myopic eye just means a “nearsighted” eye. If we draw a picture of this eye, we see that it looks big (and long) and that light focuses not onto the retina, but in front of the retina within the vitreous jelly! To correct this refractive error we use a minus (concave) lens to diverge the incoming rays of light. This effectively weakens the overall refractive power of the eye and pushes the image back onto the retina where it belongs.
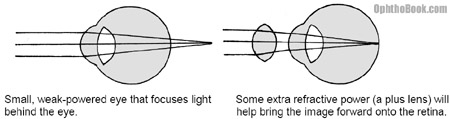
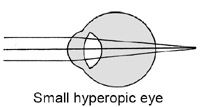
Hyperopic eyes are small, short eyes. The axial length of these eyes is so short that light focuses behind the eye. To get that image onto the retina we have to add power to the overall refractive power of the eye by using a plus (convex) lens. These convex lenses are basically your traditional magnifying glass and can make your patient’s eyes look enormous at high power.
Near-reading and Presbyopia
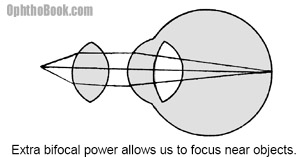
Once we get a patient corrected for distance vision we need to take care of close-up vision. With distance vision, the incoming light rays are coming in parallel before entering the eye. A near object, however, produces expanding divergent rays of light. When these rays hit the eye they end up focusing behind the eye.
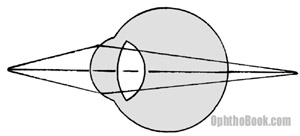
To get this near object in focus the eye needs some more refractive power. Fortunately, we are born with the natural ability to increase the strength of the lens by making it rounder. This morphing process is called “accommodation.”
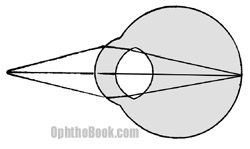
The lens works because it is suspended like a trampoline by surrounding zonular fibers. These fibers attach 360 degrees around the lens and tether the lens to the surrounding ciliary muscle. When the ciliary sphincter contracts the zonules relax and the lens becomes rounder. This rounding of the lens increases its magnification/refractive power and allows us to see near objects. With age, the lens becomes dense and does not easily round out. This presbyopia presents after age 40 and progresses with age, explaining the need for near-reading glasses in this age-group.
FUN FACT
 Unlike other vertebrates, the chameleon has a lens that is concave and actually diverges light. This works like a Galilean telescope that magnifies the retinal image compared to a traditional eye. In addition, the chameleon has a large accommodative amplitude that allows it to focus on nearby prey that roams within the field of its elastic tongue.
Unlike other vertebrates, the chameleon has a lens that is concave and actually diverges light. This works like a Galilean telescope that magnifies the retinal image compared to a traditional eye. In addition, the chameleon has a large accommodative amplitude that allows it to focus on nearby prey that roams within the field of its elastic tongue.
The chameleon uses its finely tuned monocular accommodation and evaluation of retinal size to judge distance. This is very different than the binocular stereoscopic clues that we use to judge distance.
Also, the chameleon tongue is sticky, has suction, and can even grab its prey (kind of like my leather sofa).
Implanted acrylic/plastic/silicon lenses can’t change shape at all, meaning that all post-cataract patients will need reading glasses. However, new lens are being designed to help with accommodation. Some have concentric fresnel rings that create multiple focal points (one optimized for distance and the other for near vision). Other designs work by moving the lens in an anterior/posterior direction like a telescope. Neat, huh?
Astigmatism
The cornea surface provides the majority of the refractive power of the eye. In the examples above we assumed that the cornea surface was perfectly spherical like a basketball. However, many patients have some degree of astigmatism, where the corneal surface is shaped more like a football. Thus, one axis of the cornea is steeper than the other.
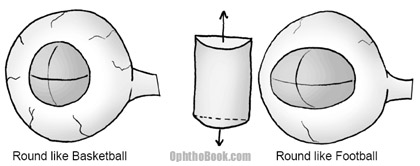
Spherical correction alone will not work for these eyes. For astigmatism, we need to add a cylindrical shaped lens to correct the refractive aberration along one axis. When we check for glasses, we determine the amount of cylinder power, and the exact angle axis this cylinder needs to be oriented to work. To measure this we use the foropter.
Using the Foropter:
The foropter is the mechanical device we use to determine glasses prescription. It’s just a big box full of lenses on dials. When manifesting a patient, we go through three steps:
1. Figure out the overall spherical error
2. Figure out the extra cylinder to correct for any
astigmatism
3. Tweak the angle of the cylinder correction
When we’re done, the foropter gives us three numbers to write down on a prescription pad:

Manifesting is a little more complicated then this, but this is enough to get us started. Let’s analyze a few sample patients and maybe this will make more sense.
Patient One
A patient hands us this prescription. He’s an engineer, and would like us to explain what the numbers mean.
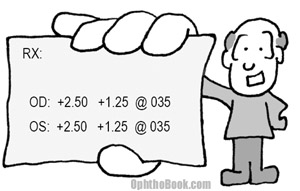
There are several parts to an eye prescription, so I’ll go through them one item at a time. The first number is the spherical error. This patient requires a +2.50 lens … this tells us that he has a small, hyperopic eye that focuses images behind the retina. He needs a little more “oomph” in his refraction to move everything forward.
The second number is the cylinder. This patient needs an additional +1.25 diopters of power to account for the steeper axis of his “football” shaped eye. The last number is the axis angle of how to orient that cylinder. His football is tilted at an axis of 35 degrees.
Patient Two
A 61 year old man presents to you with the following prescription after cataract surgery. He wants you to check the numbers to see if they make sense. What do the numbers mean?
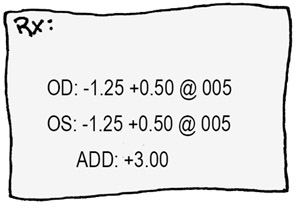
With cataract surgery we go through great pains to calculate the exact power of intraocular lens for implantation, with the desire for emetropia so that the patient doesn’t need glasses for distance. In this gentleman’s case, he is still a little myopic with a negative sphere of –1.25. We must have implanted a powerful lens implant that is focusing in the vitreous jelly. To offset this powerful implant, we need to weaken the eye by –1.25 diopters. He also has a little astigmatism of +0.50 with a cylinder angle of 5 degrees. The patient probably had this astigmatism before, but you can induce some astigmatic error via corneal incisions and sutures.
There is another number on this prescription called the “add.” This is simply the amount of extra bifocal power needed for reading. This gentleman has a plastic lens in his eye that can’t change shape at all, so he needs a +3.00 bifocal adjustment if he wants to read at approximately 1/3rd of a meter.
Patient Three
A woman brings you this prescription for her child.
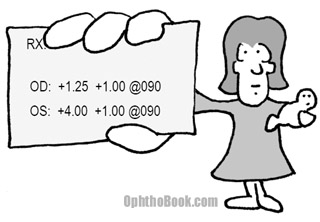
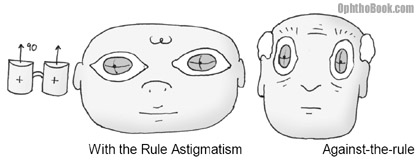
As you can see, the child is hyperopic … he must have small eyes with images focusing behind the eye. This is a common finding in infants, as their eyes are still growing. His prescription indicates he needs some plus power to pull the image forward onto the retina. In addition, the child has a little bit of astigmatism. The angle of the astigmatism is 90 degrees. We call this “with-the-rule-astigmatism” and this is common with children. With-the-rule means that corrective positive-cylinder glasses would place the cylinder axis at 90 degrees. Elderly patients often have “against-the-rule astigmatism” with their glasses having positive cylinder at an axis of 180 degrees. Here’s a picture to demonstrate what I’m talking about:
Don’t kill yourself memorizing “with the rule,” as I just wanted to familiarize you with the subject. More importantly, notice that this child has a large difference in prescription power between his eyes. This anisometropia is concerning because it can lead to amblyopia if the child begins to favor one eye over the other.
Minus or Plus Cylinder
As you’ve noticed, astigmatism can be a little confusing. It also doesn’t help that ophthalmologists and optometrists like to fix astigmatic errors differently. Ophthalmologists like to correct using a positive cylinder (which is conceptually easier in my mind) while optometrists prefer using minus cylinder (which is more useful when grinding glasses). The foropter machine comes in both flavors and your office may have both types. They both work and are conceptually the same, but with an axis that is written 90 degrees off.

Retinoscopy:
Refracting through that foropter is great, but what do you do with a child or confused patient who can’t communicate? You can actually estimate the refractive power of the eye by examining the foveal red-reflex (the red-eye you see in photographs) as you flash a light over the front of the eye. This technique is important, but tricky to perform on a child. Don’t worry too much about retinoscopy until you start your residency and have to do this yourself.
Fun Fact
The sea nautilus is a great example of eye evolution. The nautilus has neither a cornea nor a lens, but instead has a pinhole that it uses to focus light onto the retina. This concept is similar to the pinholing technique we use when checking vision and pinhole systems that are popular in spy cameras.
This pinhole eye is only a step in the evolution of the visual system: the simplist eye is merely a light-sensitive patch such as that found on the plannarium worm. This light-patch can determine light-and-dark only, with no directional component.
The next evolutionary step is to curve the eye into a bowl – since light has to get over the lip of the bowl and hits only part of the retina, this conveys some basic directional information. By closing the bowl into a pinhole (like our nautilus here) then we get fine focusing of light. The disadvantage is, of course, that only a small proportion of available light is able to get into the eye through that tiny hole. Our more advanced lens system allows focusing of much more light.
PIMP QUESTIONS
1. What bends light more — the cornea or the lens? What percentage of the eye’s total refractive power does the lens contribute?
The cornea does the majority of the refractive power of the eye, because the air-cornea interface has very different densities. The lens is only important for approximately one third of the overall refractive power of the eye.
2. A child has a cataract operation and a lens implant is inserted. A month after surgery the child sees 20/20 on the distance Snellen chart. Will this child need glasses when he returns to school?
Yes, the child needs reading glasses. An implanted plastic lens can’t accommodate (change shape) with near reading, necessitating a +3 lens or bifocal for close-up vision.
3. Your patient hands you the following prescription that they got from the optician at Wal-Mart. The prescription appears to be in minus cylinder while your favorite foropter is based on plus-power cylinder. What would be the equivalent plus cylinder prescription power for this patient?
To switch from plus to minus (or vice versa) you add the cylinder to the sphere, change the polarity of the cylinder, then change the axis by 90 degrees. Thus, the equivalent prescription for this patient is:
–3.75 + 1.50 at 005
4. A patient wants you to grind his eyeglass prescription into his SCUBA mask before his next wreck dive. Your new optical-tech has never done this before, and asks you whether she should grind the lens curvature on the inner or outer surface of the SCUBA mask. Which one is correct?
You have to grind that mask on the inside of the mask so that the lens interface is facing the mask air-bubble. A lens needs a good glass-air interface if it’s going to bend light according to Snell’s Law.
Note: this is just an example to illustrate Snell’s Law. SCUBA masks actually have inserts that are ground and placed on the inside.
5. When accommodating to view near objects, does the ciliary body relax or contract? Do the zonules get tighter or looser?
To see close-objects, the lens needs to become more powerful and get rounder. To accomplish this, the circular ciliary muscle, which is a spincter muscle, contracts. This releases tension on the zonules and the lens is allowed to become rounder.
dear Sir,
I need your help to get a 3 dimentions explaining about the meaning of Cylinder,Sphere and Axis.
thank you for your interest
Eng. Fadi Al Awad
Did anyone spell check these?? Foropter?? PHROPTER correct spelling
. . .or maybe PHOROPTER . . ?
take it easy.
great pa ji cha gai ho tussiiii ki kawan twano hun pai jan
Spelling mistakes to note:
Phoropter has a letter o before and after the r!
Re the Optics Flash Cards. Accommodation has two letter “c” and two letter “m” (have omitted the plural s as it looks silly however I type it) and as I don’t want to imply any possession, I can’t use an apostrophe! Obviously something one says rather than writes.
Worderful topic i ever enjoy during this study
Mark iga anthony ophthamology student in university of juba
i am from Tajikistan. Good jod, Thank u.
You should all be thanking Mr. Root for his amazing site, not nitpicking the spelling of terms. Great work!
Actually, isn’t the engineer’s “football”‘s axis at 125 degrees, necessitating the plus cylinder at 35 degrees?
Editors Note: Yep, but I didn’t write this out explicitly as it would sound confusing. My focus with that “example” was that astigmatism occurs at different angles than 90 and 180. I don’t find it useful for beginners to think about the shape of the eyeball “football” in too great detail, as this gets very confusing. You are technically correct, though, and I may reword this next edition.
wonderfull book short review of ophthalmology really very nice book
Thank”s for http://www.opthobook.com
How accurate and specific is the calculation for intraocular lens implants?
Can the patient expect to get specific results?
My partner, after much discussion with his surgeon, opted for a lens “just off infinity” (the surgeon’s words)so that he would be able to see extremely well in the 20-50 foot range (he’s an athlete, plays basket ball, baseball)
2 weeks following surgery, his focal length appears to be just about a meter and a half, fuzzy any further distant than 20-25 feet.
Monovision with a distance lens implanted in the second eye is NOt a good option…he needs good acuity, and most important, good depth perception.
?thoughts?
The website is very educative and i will like people from Nigeria to benefit for it.
Thank you for ur good work of inform and educating world esp. the 3rd world countries.
sir, this site is very nice n very special for learning and educating to people. nice nice nice ya its nice
i´m from brazil, resident of oftalmology
this site is very nice, learned so much, thing that i couldn´nt understand just on books ! THANKS!
hi I am optometrist and I have been learning to do biometry.
for the calculation of the IOL.
I order to do this we need the prescription of the glasses of the patient, keratometry and then the axial lens. then, the calculation of IOL can be made.
when patien has cataract usually the prescription changes and i have been reading that the appropiate prescription use for the calculation should be the one before cataract.
I feel confused how to get that prescription. my manager at the hospital say that we should use the prescription available on the clinical notes that we have at the hospital. however I think that if we do this we will always consider precription of the glasses when the patient has develop cataract.
As i have been working now in both in private practice at the community and the hospital I think that the prescription before the patient developed cataract could be requested at the practice and then have a more accurate information. what are the consequences of considering the prescription of glasses when the patient has develop cataract already?
many thanks
1.IOL calculation formula do you use? ( please show me the
equation)
2.cataract can cause myopic shift.
thanks.
dear Sir,
I need your help to get a 3 dimentions explaining about the meaning of Cylinder,Sphere and Axis as requested else where.
interested in learning optic basics
great article, thank you sir for this
hello! sir
how we can get -1.0 D against the rule astigmatism post operatively? kindly request reply.
Great info., I now know what the Prescription means! Thanks!
this site is quite awesome.’tis a good site for the populace to know more about their eyes and eyes condition. DR.ROOT,you have done a great job. more power to your elbow.
DR.EHIKPENMI O.D. (Nigeria)
this site is awesome,two thumbs up.i would like to find out what is binocular vision,what tests would one perform if the px has no binocular vision.how to perform streak retinoscopy,highlight mix astigamatism,high myopic astigmatism and aphakia.
PAUL NENANI BANDA(optometry student,zambia)
can severe astigmatism be corrected by the Intralase and Ziemer systems?
Am wondering … how much spherical power does the cylindrical portion of an Rx have? If have been told 50%.
If that’s true, then -1.00 +1.00 would be a net spherical power of -.50.
So, I’m wondering 1) if that is actually true, and 2) if the 50% would change depending on where the axis is … ?
First, Spherical Equivalent of a cylinder component is always equal to half of its value in addition to the spherical component. For example: -0.50 -4.00 x 165 will give us a Spherical Equivalent of -2.50D.
Second, it doesn’t matter what’s the axis, the value of the Spherical Equivalent won’t be affected.
Phoropter.
darcy
Dr. Root this is a wonderful training tool you have provided for students in all fields of Optometry, I am an Optician and your break down of phoria and tropia for example made it so easy to understand and absorb the topic. Thank you for your help in guiding us to become better providers to all our patients.
Hello Dr. Root ,
I am a 4th year medical student and your website helps a lot in studying the basics .
I was wondering if you could tell us something about the different angles in the eye –
The alpha , kappa , gamma and lambda angles , its too confusing .
Thankyou – your follower .
This website was of great help sir, it’s so hard to find detailed information such as yours that doesn’t make me want to sleep. This truly helped a lot, thank you sooo much! 🙂
hi there i am a resident in opthalmology
how are you?
thank you so much for sharing all of this information with us.
i am from Recife-Pe,
brazil in south america. and i love this channel.
this website i meant to say.
well
don’t ever change anything in here.
this website is wonderful. and i am about to buy your book at amazon.
when are you coming to south america to visit us down here?
look me up
Facebook
claudioagmfilho
best of luck.
and come to brazil to visit.
I have a question about hyperopia. 40 yr. old uncorrected Va distance OD 20/100 OS 20/60 but his Uncorrected near Va is
OD 20/40 OS 20/30
M OU +5.50 range Wavescan shows him +8.00 range OU
How can his near VA be this good?
I AM AN OPTOMETRIST FROM NIGERIA I MUST COMMEND THE AUTHOR. WHAT A WONDERFUL BOOK. WRITTEN WITH ALL SIMPLICITY YET INCISIVE. THANKS DOC
hello,I am final year MS student ,you make ophthal very easy.
Awesome explanation…Just got what I needed. Thanks!
Thx for the great job but I need to learn the steps of refraction , any suggested books or websites that might help?
Thank u
great info
Thank you so much for such a simple explanation for a difficult subject. You have truly helped me so much.
Thank you so much, I have been looking for a site that explains all of this in much simpler terms. I feel I have a much better understanding!!!
Hi Dr. Root,
I’ve heard of the term “spherical equivalent” and I know how it’s calculated. However, I don’t know what it is and I have a vague understanding that it’s used to calculate soft lens power and spherical glasses power. Please clarify. Thanks!
I’ve heard of the term “spherical equivalent” and I know how it’s calculated. However, I don’t know what it is and I have a vague understanding that it’s used to calculate soft lens power and spherical glasses power. Please clarify. Thanks!
I simply love it all! Thanks a lot 🙂
Hi, Dr. Timothy Root
My name is Julissa and I am an Ophthalmic Technician here in Orlando. I am from Puerto Rico and got a job as Oph Tech and I am having some problems with the refractions. Can you do a video lecture of How to Recract as the ones of Tropias vs. Phorias, Retinoscopy, and Slit lamp? There where awesome.
Thanks