
Chapter 2: Anatomy of the Eye
Before discussing conditions affecting the eye, we need to review some basic eye anatomy. Anatomy can be painful for some (personally, I hated anatomy in medical school) so I’m going to keep this simple. Let us start from the outside and work our way toward the back of the eye.
Eyelids
The eyelids protect and help lubricate the eyes. The eyelid skin itself is very thin, containing no subcutaneous fat, and is supported by a tarsal plate. This tarsal plate is a fibrous layer that gives the lids shape, strength, and a place for muscles to attach. 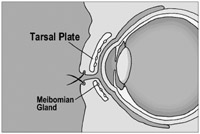
Underneath and within the tarsal plate lie meibomian glands. These glands secrete oil into the tear film that keeps the tears from evaporating too quickly. Meibomian glands may become inflamed and swell into a granulomatous chalazion that needs to be excised. Don’t confuse a chalazion with a stye. A stye is a pimple-like infection of a sebaceous gland or eyelash follicle, similar to a pimple, and is superficial to the tarsal plate. Styes are painful, while chalazions are not.
Eyelid Movement
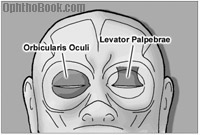
Two muscles are responsible for eyelid movement. The orbicularis oculi closes the eyelids and is innervated by cranial nerve 7. Patients with a facial nerve paralyses, such as after Bell’s Palsy, can’t close their eye and the eye may need to be patched (or sutured closed) to protect the cornea. The levator palpebrae opens the eye and is innervated by CN3. Oculomotor nerve palsy is the major cause of ptosis (drooping of the eye). In fact, a common surgical treatment for ptosis involves shortening the levator tendon to open up the eye.
CN 3 opens the eye like a pillar
CN 7 closes like a fish-hook
Conjunctiva
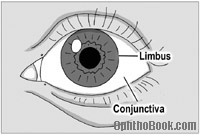 The conjunctiva is a mucus membrane that covers the front of the eyeball. When you examine the “white part” of a patient’s eyes, you’re actually looking through the semi-transparent conjunctiva to the white sclera of the eyeball underneath. The conjunctiva starts at the edge of the cornea (this location is called the limbus). It then flows back behind the eye, loops forward, and forms the inside surface of the eyelids. The continuity of this conjunctiva is important, as it keeps objects like eyelashes and your contact lens from sliding back behind your eyeball. The conjunctiva is also lax enough to allow your eyes to freely move. When people get conjunctivitis, or “pink eye,” this is the tissue layer affected.
The conjunctiva is a mucus membrane that covers the front of the eyeball. When you examine the “white part” of a patient’s eyes, you’re actually looking through the semi-transparent conjunctiva to the white sclera of the eyeball underneath. The conjunctiva starts at the edge of the cornea (this location is called the limbus). It then flows back behind the eye, loops forward, and forms the inside surface of the eyelids. The continuity of this conjunctiva is important, as it keeps objects like eyelashes and your contact lens from sliding back behind your eyeball. The conjunctiva is also lax enough to allow your eyes to freely move. When people get conjunctivitis, or “pink eye,” this is the tissue layer affected.
There is a thickened fold of conjunctiva called the semilunar fold that is located at the medial canthus – it is a homolog of the nictitating membrane seen on sharks.
Tear Production and Drainage
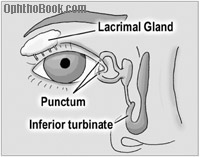 The majority of tears are produced by accessory tear glands located within the eyelid and conjunctiva. The lacrimal gland itself is really only responsible for reflexive tearing. Tears flow down the front of the eye and drain out small pores, called lacrimal punctum, which arise on the medial lids. These puncta are small, but can be seen with the naked eye.
The majority of tears are produced by accessory tear glands located within the eyelid and conjunctiva. The lacrimal gland itself is really only responsible for reflexive tearing. Tears flow down the front of the eye and drain out small pores, called lacrimal punctum, which arise on the medial lids. These puncta are small, but can be seen with the naked eye.
After entering the puncta, tears flow down the lacrimal tubing and eventually drain into the nose at the inferior turbinate. This explains why you get a runny nose when you cry. In 2-5% of newborns, the drainage valve within the nose isn’t patent at birth, leading to excessive tearing. Fortunately, this often resolves on it’s own, but sometimes we need to force open the pathway with a metal probe.
Lid Lacerations
 Most lacerations through the eyelid can be easily reaproximated and repaired. However, if a laceration occurs in the nasal quadrant of the lid you have to worry about compromising the canalicular tear-drainage pathway. Canalicular lacerations require cannulation with a silicone tube to maintain patency until the tissue has healed.
Most lacerations through the eyelid can be easily reaproximated and repaired. However, if a laceration occurs in the nasal quadrant of the lid you have to worry about compromising the canalicular tear-drainage pathway. Canalicular lacerations require cannulation with a silicone tube to maintain patency until the tissue has healed.
Warning: Drug absorption through the nasal mucosa can be profound as this is a direct route to the circulatory system and entirely skips liver metabolism. Eyedrops meant for local effect, such as beta-blockers, can have impressive systemic side effects when absorbed through the nose. Patients can decrease nasal drainage by squeezing the medial canthus after putting in eyedrops. They should also close their eyes for a few minutes afterwards because blinking acts as a tear pumping mechanism.
The Eyeball:
 The eyeball is an amazing structure. It is only one inch in diameter, roughly the size of a ping-pong ball, and is a direct extension of the brain. The optic nerve is the only nerve in the body that we can actually see (using our ophthalmoscope) in vivo.
The eyeball is an amazing structure. It is only one inch in diameter, roughly the size of a ping-pong ball, and is a direct extension of the brain. The optic nerve is the only nerve in the body that we can actually see (using our ophthalmoscope) in vivo.
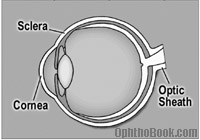
The outer wall of the eye is called the sclera. The sclera is white, fibrous, composed of collagen, and is actually continuous with the clear cornea anteriorly. In fact, you can think of the cornea as an extension of the sclera as they look similar under the microscope. The cornea is clear, however, because it is relatively dehydrated. At the back of the eye, the sclera forms the optic sheath encircling the optic nerve.
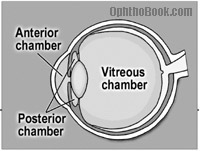 The eyeball is divided into three chambers, not two as you might expect. The anterior chamber lies between the cornea and the iris, the posterior chamber between the iris and the lens, and the vitreous chamber extends from the lens back to the retina.
The eyeball is divided into three chambers, not two as you might expect. The anterior chamber lies between the cornea and the iris, the posterior chamber between the iris and the lens, and the vitreous chamber extends from the lens back to the retina.
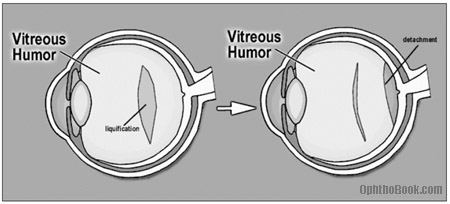
The eye is also filled with two different fluids. Vitreous humor fills the back vitreous chamber. It is a gel-suspension with a consistency similar to Jell-O. With age and certain degenerative conditions, areas of the vitreous can liquefy. When this occurs, the vitreous can fall in upon itself – usually a harmless event called a PVD (posterior vitreous detachment). However, this normally benign vitreous detachment can sometimes tug on the retina and create small retinal tears.
Aqueous humor fills the anterior and posterior chambers. This is a watery solution with a high nutrient component that supports the avascular cornea and lens. Aqueous is continuously produced in the posterior chamber, flowing forward through the pupil into the anterior chamber, where it drains back into the venous circulation via the Canal of Schlemm. We’ll discuss the aqueous pathway in detail in the glaucoma chapter.
The Cornea:
The cornea is the clear front surface of the eye. The cornea-air interface actually provides the majority of the eye’s refractive power. The cornea is avascular and gets its nutrition from tears on the outside, aqueous fluid on the inside, and from blood vessels located at the periphery.
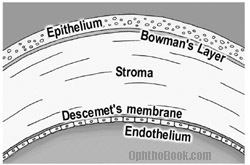
On cross section, the cornea contains five distinct layers. The outside surface layer is composed of epithelial cells that are easily abraded. Though epithelial injuries are painful, this layer heals quickly and typically does not scar. Under this lies Bowman’s layer and then the stroma. The corneal stroma makes up 90% of the corneal thickness, and if the stroma is damaged this can lead to scar formation. The next layer is Descemet’s membrane, which is really the basal lamina of the endothelium, the final inner layer.
The inner endothelium is only one cell layer thick and works as a pump to keep the cornea dehydrated. If the endothelium becomes damaged (during surgery or by degenerative diseases) aqueous fluid can flow unhindered into the stroma and cloud up the cornea with edema. Endothelial cell count is very important as these cells don’t regenerate when destroyed – the surviving endothelial cells just get bigger and spread out. If the cell count gets too low, the endothelial pump can’t keep up and the cornea swells with water, possibly necessitating a corneal transplant to regain vision.
Decemet’s membrane is “deep,” while Bowman’s layer is high up in the “belfry.” A belfry is a room, usually high up in a tower, where bells are hung.
The Anterior Chamber Angle
T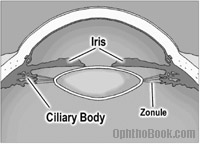 he angle formed by the inner cornea and the root of the iris is particularly important in ophthalmology. Here you find the trabecular meshwork with its underlying Schlemms Canal. This is where aqueous is drained, and blockage of this pathway/angle will become important as we discuss glaucoma.
he angle formed by the inner cornea and the root of the iris is particularly important in ophthalmology. Here you find the trabecular meshwork with its underlying Schlemms Canal. This is where aqueous is drained, and blockage of this pathway/angle will become important as we discuss glaucoma.
The Uvea (iris, ciliary body, choroid)
 The iris, ciliary body, and the choroid plexus are all continuous with each other and are collectively called the uvea. This is an important term, as many people can present with painful “uveitis” – spontaneously or in associated with rheumatologic diseases.
The iris, ciliary body, and the choroid plexus are all continuous with each other and are collectively called the uvea. This is an important term, as many people can present with painful “uveitis” – spontaneously or in associated with rheumatologic diseases.
The iris is the colored part of the eye and its primary function is to control the amount of light hitting the retina. Sympathetic stimulation of the pupil leads to pupil dilation and parasympathetic stimulation leads to constriction. In other words, if you see a bear in the woods, your sympathetics kick in, and your eyes dilate so you can see as much as possible as you run away. I’ll be using this mnemonic/metaphor many times throughout this book to help you remember this concept.
The inner iris flows back and becomes the ciliary body. The ciliary body has two functions: it secretes aqueous fluid and it controls the shape of the lens. The ciliary body contains sphincter muscles that change the lens shape by relaxing the zonular fibers that tether to the lens capsule.
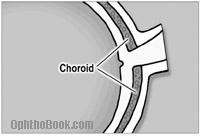
The choroid is a bed of blood vessels that lie right under the retina. The choroid supplies nutrition to the outer one-third of the retina which includes the rod and cone photoreceptors. Retinal detachments can separate the retina from the nutritious choroid, which is disastrous for the photoreceptors as they quickly die without this nourishment.
FUN FACT:
An ostrich’s eye is larger than its brain.
Lens:
The lens sits behind the iris. The lens is unique in that it doesn’t have any innervation or vascularization. It gets its nourishment entirely from nutrients floating in the aqueous fluid. The lens also has the highest protein concentration of any tissue in the body (65% water, 35% protein).
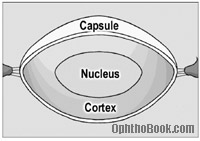
The lens has three layers in a configuration similar to a peanut M&M. The outer layer is called the capsule. The capsule is thin with a consistency of saran wrap and holds the rest of the lens in place. The middle layer is called the cortex, while the central layer is the hard nucleus. Cataracts are described by where they occur such as nuclear cataracts, cortical cataracts, and subcapsular cataracts. With cataract surgery the outer capsule is left behind and the artificial lens is placed inside this suporting bag.
The capsule is held in place by suspensory ligaments called zonules that insert around the periphery and connect to the muscular ciliary body. Contraction of the ciliary muscle causes the zonule ligaments to relax (think about that for a minute), allowing the lens to become rounder and increase its refracting power for close-up reading.
In children the lens is soft but with age the lens hardens and becomes less pliable. After age 40 the lens starts having difficulty “rounding out” and people have problems focusing on near objects. This process is called presbyopia. Almost everyone over 50 needs reading glasses because of this hardening of the lens.
The Retina:
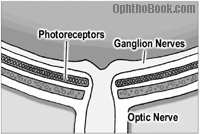
The retina is the sensory portion of the eye and contains layers of photoreceptors, nerves, and supporting cells. Histologically, many cell layers can be seen, but they are not worth memorizing at this point. The important ones include the photoreceptor layer, which is located further out (towards the periphery), and the ganglion nerve layer which lies most inward (toward the vitreous). For light to reach the photoreceptor it has to pass through many layers. After light reaches the photoreceptors the visual signal propagates back up to the ganglion nerves. These ganglion nerves, in turn, course along the surface of the retina toward the optic disk and form the optic nerve running to the brain.
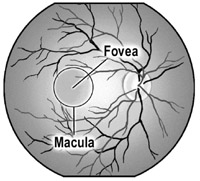 The macula is the pigmented area of the retina that is responsible for central vision. Within the central macula lies the fovea, which is a small pit that is involved with extreme central vision. The fovea is very thin and derives its nutrition entirely from the underlying choroid, making it susceptible to injury during retinal detachments.
The macula is the pigmented area of the retina that is responsible for central vision. Within the central macula lies the fovea, which is a small pit that is involved with extreme central vision. The fovea is very thin and derives its nutrition entirely from the underlying choroid, making it susceptible to injury during retinal detachments.
The optic disk is the entry and exit point of the eye. The central retinal artery and vein pass through here, along with the the ganglion nerves that form the optic nerve. A physiologic divot or “cup” can be found here that will become important when we talk about glaucoma.
The Orbital Walls:
Seven different bones form the orbital walls: don’t be intimidated by this complexity, however, as these bones are not that confusing when you break them down. For example, the roof of the orbit is a continuation of the frontal bone, the zygomatic bone forms the strong lateral wall, while the maxillary bone creates the orbital floor. This makes sense, and you could probably guess these bones from the surrounding anatomy.
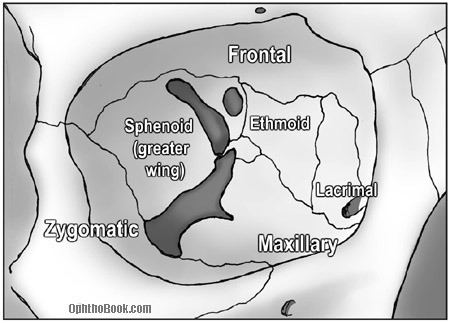
The medial wall is a little more complex, however, but is mainly formed by the lacrimal bone (the lacrimal sac drains tears through this bone into the nose) and the ethmoid bone. The thinnest area in the orbit is a part of the ethmoid bone called the lamina papyracea. Sinus infections can erode through this “paper-thin wall” into the orbital cavity and create a dangerous orbital cellulites.
Despite the fragility of the medial wall, it is well buttressed by surrounding bones, such that it’s the orbital floor that breaks most often during blunt trauma. The maxillary bone fractures downward and the orbital contents can herniate down into the underlying maxillary sinus. This is called a “blowout fracture” and can present with enopthalmia (a sunken-in eyeball) and problems with eye-movements from entrapment of the inferior rectus muscle. We’ll discuss blow-out fractures in more detail in the trauma chapter.
The back of the orbit is formed by the greater wing of the sphenoid bone, with the “lesser wing” surrounding the optic canal. There’s also a little palatine bone back there in the middle, but don’t worry about that one!
The Apex: Entrance into the Orbit
The orbital apex is the entry point for all the nerves and vessels supplying the orbit. The superior orbital fissure lies between the wings of the sphenoid bones, through which many vessels and nerves pass into the orbit.
The “Annulus of Zinn,” a muscular band that serves as the insertion point for most of the ocular muscles, rests on top of the superior orbital fissure. The four rectus muscles attach to the annulus and the optic nerve passes right through the middle.
Eye Muscles:
Four rectus muscles control each eye. These muscles insert at the sclera, behind the limbus, and each pull the eye in the direction of their attachment.
The superior, medial, and inferior rectus muscles are all controlled by the oculomotor nerve (III). The lateral rectus, however, is controlled by the abducens (VI) nerve, which makes sense as the lateral rectus “abducts” the eye.
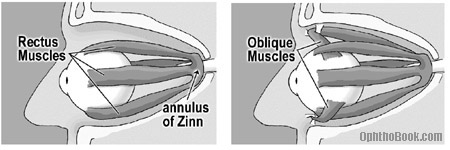
The remaining two eye muscles are the superior and inferior oblique muscles. The superior oblique also originates in the posterior orbit, but courses nasally until it reaches the trochlea (or “pulley”) before inserting onto the eye. The inferior oblique originates from the orbital floor and inserts behind the globe near the macula. Because of these posterior insertions, the oblique muscles are primarily responsible for intorsion and extorsion (rotation of the eye sideways), though they also contribute some vertical gaze action.
Confused, yet? Don’t kill yourself learning the action of the oblique muscles or nerve innervation as we’ll discuss these topics in greater detail in the neurology chapter.
Summary:
There is much more anatomy we could cover, but let’s hold off for now and discuss more detailed anatomy in future chapters as they become relevant.
PIMP QUESTIONS
1. Why don’t objects like contact lens and eyelashes get stuck behind the eye?
Because the conjunctiva covering the front of the eye loops forward and covers the inside of the eyelids as well.
2. How many chambers are there in the eyeball?
Three, actually. The anterior chamber sits in front of the iris, the posterior chamber between the iris and the lens, and the vitreous chamber lies behind the lens filling most of the eye.
3. Name each of the numbered bones.
Which bone is thinnest?
Which is most likely to fracture after blunt injury?
Which is most likely to erode from sinus infections?
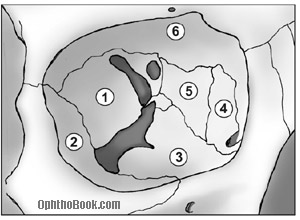
The bones are: (1)Sphenoid (2)Zygomatic (3)Maxilla (4)Lacrimal (5)Ethmoid (6)Frontal. The ethmoid is the thinnest bone and most likely to perforate from an eroding sinus infection (this happens mostly in kids). The maxillary floor is most likely to fracture from blunt injury.
4. What is the uvea? What eye structures compose it?
The uvea comprises the iris, ciliary body, and the choroid. They are all connected to each other and are histologically similar. Patients can present with a painful “uveitis,” an inflammation of the uvea, often secondary to rheumatological/inflammatory conditions like sarcoidosis.
5. Where does the retina get its nutrition supply?
The inner 2/3rds of the retina (inner implies toward the center of the eyeball) gets its nutrition from the retinal vessels. The outer 1/3 (which includes the photoreceptors) is nourished by the underlying choroid plexus. A retinal detachment, which separates the retina from the choroid, is particularly dangerous for the photoreceptors. This is especially true for detachments involving the macula as the thin macula gets its blood supply primarily from the underlying choroid.
6. When the ciliary body contracts, how does the lens change shape (does it get rounder or flatter)?
The ciliary body is a round, spincter-like muscle, so when it contracts the zonules actually relax, allowing the lens to relax and become rounder. With age, the lens hardens and has a hard time relaxing, no matter how hard the ciliary muscle contracts. This aging process is called presbyopia.
7. Which extraocular muscle doesn’t originate at the orbital apex?
Unlike the other muscles, the inferior oblique originates from the orbital floor before inserting on the back of the globe near the macula.
8. Which full-thickness eyelid laceration is more dangerous – medial or lateral lacerations? Why?
You worry about the canalicular tear-drainage system involvement with medial lacerations. You want to repair this system as soon as possible, to avoid chronic epiphora.
9. How many layers are there in the cornea? Can you name them?There are five: the superficial Epithelium, Bowman’s layer, Stroma, Decemet’s membrane, and the inner Endothelium.
10. How does the water content of the cornea differ from the rest of the eye?
The cornea is relatively dehydrated, which helps with clarity. If water gets into the cornea, via a disrupted endothelium or a high pressure gradient from acute glaucoma, the cornea turns hazy and white.
11. A pseudophakic (i.e. implanted lens) patient is found to have excellent far vision, but reading is terrible. What’s going on?
As we get older, our natural lenses harden and do not change shape very well making it hard to accommodate and see near objects. This phenomenon is called presbyopia and is a normal finding in people over 40 years of age. A prosthetic lens is not able to change shape at all, so all patients (including small children) with implanted plastic lenses require reading glasses to read.
truly commenting, the ophthobook.com could serve an indespensable material for writing thesis on Ocular anatomy. Wish copies could be made avaialable, while a reply is awaited via the E-mail address. Thn x
ophthobook.com is a very useful site for optom students-very handy!
i am studdying sharks in school and i cannot seem to find what is the nasal canthus?
The nasal canthus is where the medial eyelids come together and attach to the bone next to the nose.
the website has given facts other then usual textbook. authors sincere efforts towards presentation are worth to applause. however i would surely suggest site for best ophthlmology edutainer site.
Very useful and didactic! Congratulations on your good work!
OphthoBook.com is an impressively well organized, concise review of clinically relevant Ophthalmology. We have selected OphthoBook.com as one of our featured links on our Ophthalmology Links page.
Nicely done!
-The MedZoom Team
http://www.medzoom.net
very useful for every medical person
thx guys………u helped me pass my optho exam…………….cheers………
i love thiss! its so awesome. watched the video before my exam woo!
My sister has swelling of the optic nerve, it has got better recently but a new problem has occured, they have told us there are three layers of the eye and the two outer layers are breaking away from eachother. can you explain this to me and will she go blind?
Hi!
The American Association for Pediatric Ophthalmology and Strabismus would like to use your orbital bone anatomy diagram in its discussion about orbital fractures. May we have your permission to do so (we will give you full credit on the page and use the image as is)?
Thank you!
David Epley
It is good for every body
Thank
mark Iga anthony
Hi..,
this was really important me to do my exams well….! this was really useful.
Thank you
I am medicine student and i got ur website through ur videos in the youtube.com, to be hosnet ur viedos is imazing and explain much better than any book i have read it, hope u can lunch more videos about the eys and eye problems and stuff that can be useful for medical students(first year).
And i have one question, My mom see a black line where ever she look(only if she look at a white wall or anything not dark,she can see a black line,thats move anywhere she look and is in the same place always, what does that mean do u think?)
Thank you alot.Regards
Terrific! Finally we found what we were looking for. Thanks!
easy to watch easy to read easy to understand !! great book, great doctor, great website …..
mecca , SA
i want anatomy of sclera
This is probably the best book I have ever encountered when looking for an easy to understand book.
thanks soooooooo much
great job u have done
u are the best
thanks again
can’t tank you enough for this!God bless u!
medical student.
hi,
i am an optom.it’s very usefull for optom.Or students.
i am thankfull to ur team.
thanks ophthobook.com
I am working as a scrub nurse and I often work with eye surgeons. I would like to say thank you for creating this website where I can read and understand anything about the eye and you made it very interesting that I can understand it easily.
Again my appreciation.
awesome site.
Sir,
Thanks.
It’s really a fantastic site.
I enjoyed very much and share with my students.
One things I like to mention here for your kind attention that choroid plexus might be a printing mistake. Choroid plexus locate in Ventricles of CNS and Choroid is a part of uveal tract.
Again thanks to you.
Razu
very nice presntation
thanks
thanks this information.if you have about squaint(eye)how to diognes clinicaly.thanks joing me.
This is truly an amazing website!
I have always found anatomy of the eye the most toughest of all , and now that i am in my Final Year of MBBS this has helped me a lot to clear my concepts, once again.
Awesome work!
I’m gonna be examined in 4 days – this is heaven!!! Love it already!
Thank you so much for this wondreful reference and the hard work put in it. I truly appreciate it as an optometry student
Hi
It is wonderful and I put it a favourite link .
Thank you
regards
Dr Rasuly
U.K
thanks its really help me for my dot study
This is the first time I have understood the anatomy of the eye. Thank you.
ايه هية Tarsal plate ?
CAN YOU GO BLIND FROM MEIOBIAN GLand DISEASE???
Wow! I’m going to begin my opthalmology rotation soon and this is an amazing read so that I don’t look completely ridiculous, thank you so much for making this so incredibly clear and consise! You have done such a wonderful service to all of us students, thanks so much!
just what i need…thanks
god bless you
thank you.
This is concise, clear and oh-my-god-I’ve-finally-understood-the-goddamn-eye!!! You’ve just saved me! My ophthalmolgy exam’s next week and I was terrified, I didn’t even understand the basic structures. Thank you, thank you, thank you, you’re wonderful.
Vry nice this iz vry helpful for my study
useful and simple to understand!!!
useful and simple to understand!!!
saved me from my ophtho proff!!!
Great site found by accident will tell my peers
useful and simple to understand!!!
saved me from my ophtho proff!!!
nice and easy .makes ophthalmology understandable.thanks…..
how to remember the embryological development of the eye structures?
I feel inspired to pursue ophthalmology now that the foundation has been made more approachable and interesting! Excellent teaching!
Wow!!! I love that,concised and detailed.Highly recommended for optometrists like myself….keep it up
I am an emergency physician and arrived at your page whilst working on a lecture. Can you tell me why some parts of the eye are insensate? I imagine feeling arterial pulsation in the eye may be an elovutionary reason and obviously the external eye needs to be sensate. But why would the pupillary apparatus be sensate whilst the sclera not?
I agree with other readers – a nice site, thank you.
Wow! This is indeed a valuable basic eye anatomy note. It is user friendly and easy to understand. Thanks to the authors.
Now there are 6 layers in the cornea including the Duo’s layer
i want this book to be available in every market but in affordable price 🙁
Gud info for optometry students lyk me
bravo!
I have noticed small white lines on just the upper perifery of my both eyes’ irises for a month.Are those a symptom of a desease ?
I would be grateful if responded.
Mehmet
Mehmet, you may be seeing some lines of “arcus senilis.” If it is changing, however, or having vision decrease/pain … see an eye doctor to confirm.
Thank you Mr.Root;I’ll keep watching “arcus senilis “
I am interested in why the lens becomes stiffer as we age. Cross-linking polymers perhaps?
Informative and easy to read!Thank you!
really just super explanations! Thanks so much for providing this! Your explanations took all the stress out of understanding the eye. They were wonderful and seemed to include EVERYTHING but your manner of explaining and organizing the material was so clear, it really made things easy to understand. Thanks so much!!
thank you you helped me a lot!!!!!!!! now i wont fail this test
Its a very useful site for the medical students. Also the GPs can also take benefit from it. Tom really made an enormous
effort in the field of Health Education.
Its a very useful site for the medical students. Also the GPs can also take benefit from it. Tom really made an enormous
effort in the field of Health Education. The A&E staff should study all the stuff and they will really get benefit to serve the humanity very well.
Regards.
I would like to say thank you for creating this website where I can read and understand anything about the eye and you made it very interesting that I can understand it easily.
its truly very useful for bs.c optomatory
Really it’s one of the best guide line 4 ophtalmology students……
excellent teachingcapacity. nothingtosaymore. godblessthenarrator. iamgrateful.thanks.
Eureka I have found everything I needed.Thanks a lot I now understand what i was taught
Really really helpful. I’m a nurse practitioner student and this is a great website for EYES!
Am a new student in optometry, my lecturer asked all students to be presenting each topic and am the first. My topic is uvea which is the middle vascular coat of eyebal. Please can explain to me how to present. Thanks
I’m a nursing student, who is currently studying vision, your site is great. Love the jokes! A sense of humor while studying is a must!
I just found your videos while studying for my exam. They are fun, straight to the point, easy to follow. Thank you so much for making it interesting, fun and understandable. Keep up the good work 😉
Useful material help me to complete my presentation to community keep it up to reduce blindness due low knowledge
Its very useful for me ,thank u…
Thanks .useful to me
this is just awesome …added to my favourites <3
It was very usefull to me because i like too much Ophthalmology to read.
Thank you very much……..
Really it is agreat book as they said
I am going to school to become a surgical tech. I came here for a little bit of info about anatomy and ended up reading the whole thing. It is so interesting, thanks!!
i have a doubt that why does the extraocular muscles insertion into the sclera is not visible to the naked eye??
Is cornea behind conjunctiva? I am a bit confused.
the conjunctiva is the “clear skin over the eye” and it covers the anterior surface, excluding the clear cornea
what does the fat behind the eye do
Its so awesome…
Its used for all medical student
Great site, I am an computer animation artist studying gaze motion of the eye. Just learned about Listing’s and Donder’s laws. Do you know if a healthy eyeball (sclera) deforms (squishes) due to the forces of the rectus muscles? My hunch is yes (that the sclera changes shape as the eye abducts/adducts).
Also do the eyes remain perfectly yoked during extreme dextroversion or levoversion, or does can one eye get more fatigued than the other and not keep up?
Thanks for providing a free resource for students. I will be encouraging my medical students to review your book as they rotate through our ophthalmology clinic. David George, MD
I really would like to thank you.
From a ophthalmology resident.
Well done on the presentation. Appropriate use of humour. (I suspect you have a wicked Sense of Humour when unleashed!! LOL! )
Great general revision for an old hat like myself.
Looking forward to further reading..
amazing explanation!!
could you explain the iris shadow? why do we see it in immature cataract but not in mature cataract?
A great ..awesome…simple …informative
The mitochondria is the powerhouse of the cell; Tim Root is the powerhouse of medical students learning ophthalmology.